 |  |
As surgical technology evolves, the number of options we have to improve post-cataract vision continues to grow. FDA approval seems imminent for the IC-8 intraocular lens (IOL) from AcuFocus, which stands out among the rest by combining small-aperture optics with a monofocal lens. This lens adds a small mini-ring in its center that extends depth of focus. The lens is designed to mitigate the visual effects of unfocused peripheral light.
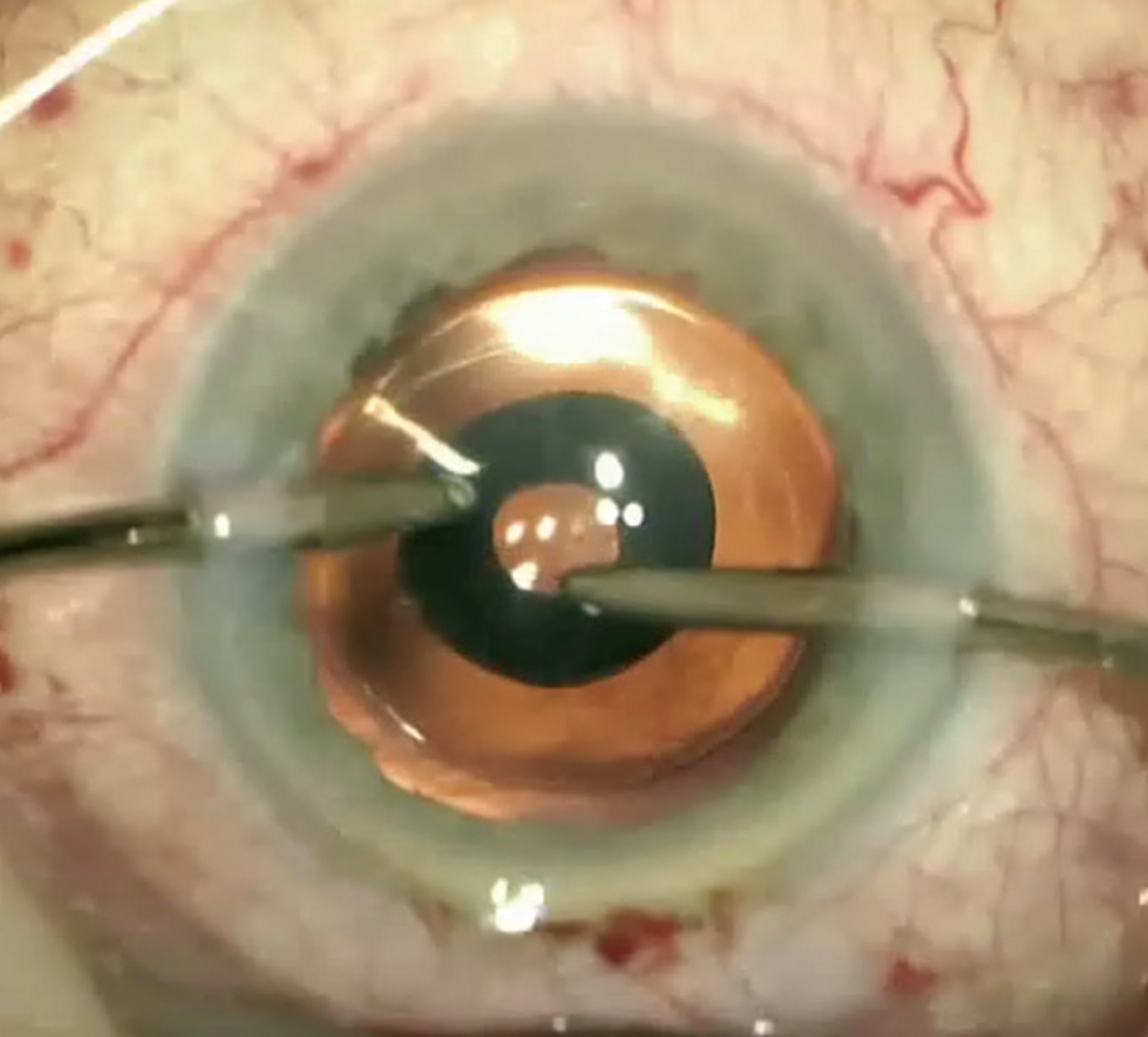 |
| The mini-ring in the center of the IC-8 IOL extends a patient’s depth of focus. Photo: H.B. Dick, PhD, MD, and T. Schultz, MD. Click image to enlarge. |
Range of Benefits
The 1.36mm aperture of the ring only allows focused rays of light onto the retina, while the peripheral, defocused rays are blocked by the 3.23mm mask, a descendant of the now-discontinued Kamra corneal inlay. It is a one-piece hydrophobic, acrylic IOL with a 6mm optic zone, 12.5mm length and powers that range from +10D to +30D in 0.50D steps.
A toric design has not been released; however, the IOL can work for up to 1.50D of astigmatism due to the pinhole effect. The lens has been reported to provide up to 3D of extended depth of focus with a monovision offset, reduce effects of lower and higher-order aberrations and allows plus or minus 1D of deviation from target refraction.
Implanting the Lens
In most cases, the IC-8 lens is used in combination with a low amount of monovision, typically -0.75D to -1D. The lens is implanted in the non-dominant eye and a monofocal IOL with an aim of plano is placed in the dominant eye. Assuring the lens is well-centered with the visual axis to allow the optics to work properly is important.
Also, refracting these patients can yield interesting results due to the extended depth of focus. For this reason, a midpoint refraction or a red/green balance refraction is recommended. For the midpoint refraction, begin with a manifest refraction, then determine the maximum plus and maximum minus lenses to blur, and then determine the midpoint. For the red/green balance refraction, you want the patient to report the letters on the green and red side being equal in clarity.
Surgeons have reported good near and intermediate vision with better distance vision compared to traditional monovision. There is also less ametropia due a lower amount of offset for the IC-8 IOL eye.
Who Can Benefit from IC-8?
Patients with irregular corneas from keratoconus or previous refractive surgeries such as radial keratotomy could benefit from this lens because only central light rays reach the retina. However, due to the reduced amount of light entering the light with this modality, it is important to be cautious if considering implanting bilaterally. The lens may also be beneficial in those reporting light sensitivity or problems with glare.
Patients with central corneal scarring, large pupils, macular pathology, severe glaucoma, AMD, vitreous opacities or even those with high need for near vision should not be considered candidates for this IOL. Patients with pupils larger than the mask can notice dysphotopsias. Reduced contrast sensitivity can occur, as well as a minor reduction in visual field. Patients may report difficulties in low-light conditions due to the IOL design.
Postoperative management is fairly similar to other IOLs with a few extra considerations, including thorough patient education on this type of lens modality, which will provide a smoother postoperative period.
From patients desiring presbyopia correction to those looking for greater functional range of vision, this unique IOL should provide solutions for appropriately selected and properly educated patients.
Dr. Cunningham is the director of optometry at Dell Laser Consultants in Austin, TX. He has no financial interests to disclose. Dr. Whitley is the director of professional relations and residency program supervisor at Virginia Eye Consultants in Norfolk, VA. He is a consultant for Alcon. Dr. Wysiadlowski is an ocular disease resident at Dell Laser Consultants in Austin, TX.
