 |
Q: A 60-year-old white male reported decreased vision and pain in his left eye that persisted for about two months. The patient recently had an episode of complete loss of vision, which returned after about 30 seconds. Dilated fundus examination revealed mid-peripheral retinal hemorrhages 360° in the left eye. What do I need to be mindful of regarding this patient?
A: “This patient seems to be exhibiting signs and symptoms of ocular ischemic syndrome,” says Trennda Rittenbach, OD. It’s not a common condition, but she sees it often at the Palo Alto Medical Foundation in Sunnyvale, Calif.
The most frequent symptom of ocular ischemic syndrome (OIS) is vision loss in the affected eye, which is present in more than 90% of patients with OIS; about 67% have a gradual vision loss over a few weeks to months, Dr. Rittenbach says.1 Other common symptoms include episodes of transient vision loss (amaurosis fugax), peripheral vision loss and pain.1
Signs of OIS are narrowed retinal arteries, beaded and dilated veins with tortuosity, dot-and-blot hemorrhages and microaneurysms located in the mid-peripheral retina (which may extend to the posterior pole as hypoxia increases), cotton-wool spots, anterior ischemic optic neuropathy, rubeosis iridis, iris atrophy and asymmetric cataract.1,2
|
|
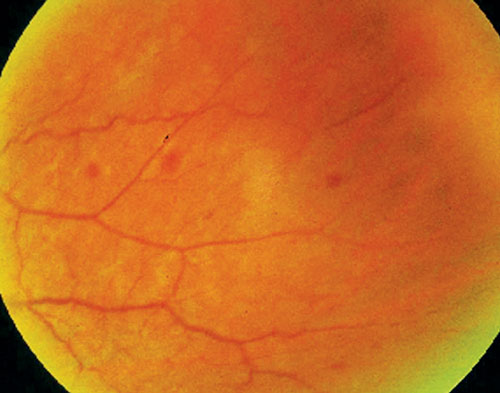
| Mid-peripheral retinal hemorrhages are common in ocular ischemic syndrome. Photo: Joseph J. Pizzimenti, OD |
|
Differential diagnoses of OIS include diabetic retinopathy (which is often confused for OIS), hypertensive retinopathy and a mild or moderate central retinal vein occlusion.
“OIS occurs when stenosis or occlusion of the carotid arteries causes ocular hypoperfusion,” Dr. Rittenbach says.2 “The hypoperfusion puts the eye in a hypoxic state, leading to attenuated arteries, venous tortuosity and mid-peripheral hemorrhages.”
Atherosclerosis is usually the main underlying cause for the changes in the carotid arteries, Dr. Rittenbach says, adding that she diagnosed OIS in a patient recently. “I dug deeper into his medical history and found that he already had a carotid endarterectomy on his right side and a history of atherosclerosis,” she says.
She performs auscultation on every patient she suspects has a carotid artery occlusion problem, but acknowledges that the sensitivity and specificity of auscultation of the carotid arteries is not definitive.
“Also during initial examination, be sure to look closely for an important complication secondary to OIS: neovascularization of the iris, which can lead to neovascularization glaucoma,” she says.
Management of the patient with OIS includes ordering a lipid panel for hypercholesterolemia, as well as a bilateral carotid ultrasound. “It is an absolute must to rule out giant cell arteritis, so I always order a complete blood count with differentials to see if there is evidence of thrombocytosis related to GCA, as well as a sedimentation rate and C-reactive protein,” she says.
“The five-year mortality rate is as high as 40% in patients diagnosed with OIS,” Dr. Rittenbach says.3 “So, these patients must be comanaged with a vascular surgeon, cardiovascular physician or primary care physician.”
For her own recent experience with an OIS patient, Dr. Rittenbach ordered a carotid ultrasound and referred him back to his vascular physician for consideration of carotid endarterectomy, pending the ultrasound results. Also, in her referral letter, she noted that this patient’s blood pressure was 158/86mm Hg, which needs to be addressed.
Remember, as a health care provider, you should check blood pressure on all your patients, day in and day out.
1. Terelak-Borys B, Skonieczna K, Grabska-Liberek I. Ocular ischemic syndrome - a systematic review. Med Sci Monit. 2012 Aug;18(8):RA138-44.
2. Lyons-Wait VA, Anderson SF, Townsend JC, De Land P. Ocular and systemic findings and their correlation with hemodynamically significant carotid artery stenosis: A retrospective study. Optom Vis Sci. 2002 Jun;79(6):353-62.
3. Hazin R, Daoud YJ, Kahn F. Ocular ischemic syndrome: recent trends in medical management. Curr Opin Ophthalmol. 2009 Nov;20(6):430-3.
