 |
Q:
I have a 47-year-old patient who has noticed a rapid decline in vision in his right eye since beginning chemotherapy with Sprycel (dasatinib, Bristol-Myers Squibb) for leukemia. Best-corrected acuity is 20/50 OD with some nuclear sclerosis, but my view of the fundus is crystal clear. What else could it be?
A:
Even when you have found nuclear sclerosis to be the cause of the patient’s vision loss, don’t underestimate it. “Milky nuclear sclerosis has a way of hiding in plain sight,” says Heather Purman, OD, of Omni Eye Services of Atlanta. Without any yellowing or brunescence, the cataract has the appearance of a white lens within a lens and is often unilateral. “Most of us were taught that our view into the eye is associated with the patients view out when it comes to cataracts, but not with milky nuclear sclerosis,” Dr. Purman says.
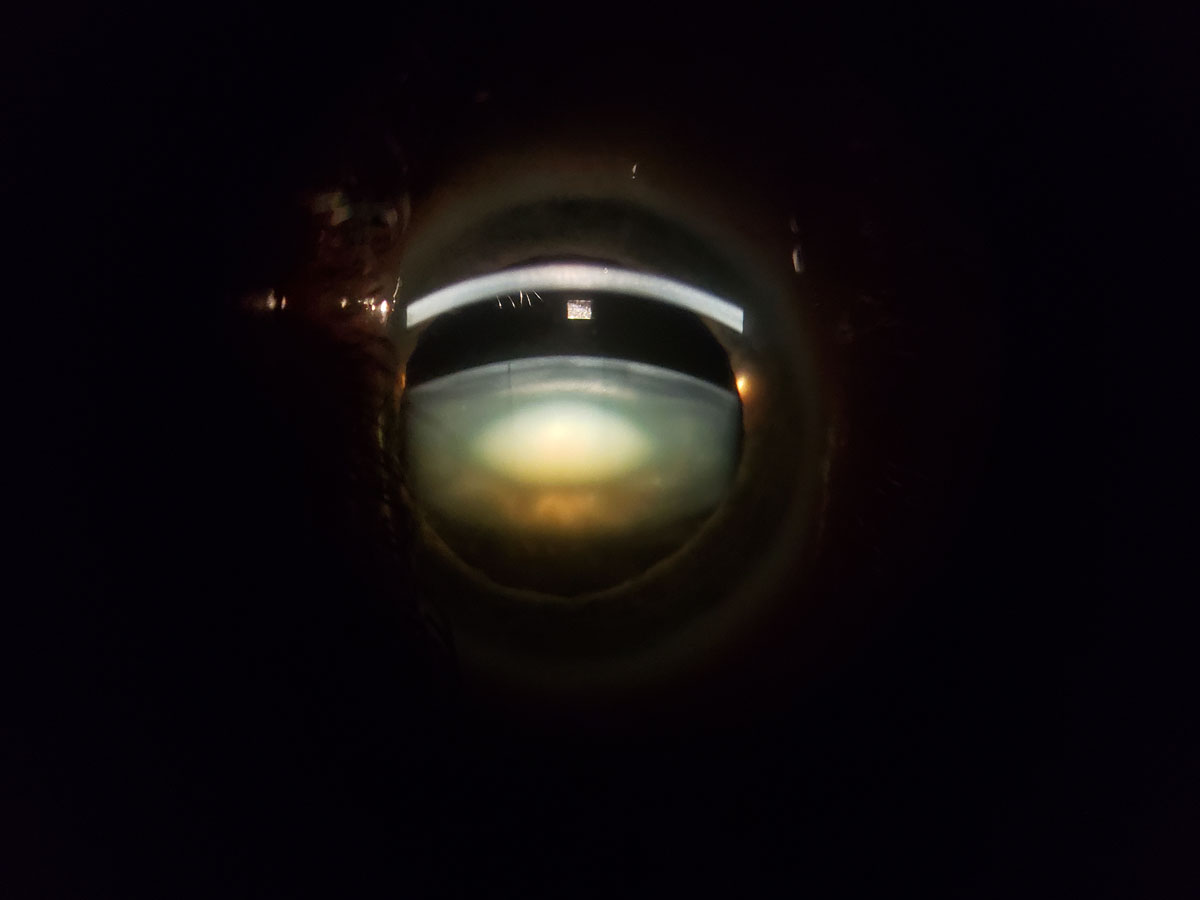 |
| A sudden, large unilateral myopic shift could suggest milky nuclear sclerosis. Click image to enlarge. |
Avoid Over-referrals
Other findings to look for with milky nuclear sclerosis are myopic shift, bowing of the light beam on fundus exam and a dark reflex centrally on retinoscopy. In a similar case, a 44-year-old patient presented with decreased vision in his right eye that happened rapidly, with a medical history of trauma to the right side of his head. Initially Dr. Purman thought it could be a traumatic cataract, but upon further examination, the patient had a six diopter myopic shift OD and best-corrected acuity of 20/100 OD and 20/20 OS.
On slit lamp exam, the patient had 4+ milky nuclear sclerosis OD and a clear lens OS. The fundus exam was unremarkable, and the patient was referred for removal of the cataract. At the one day post-op visit, the patient was 20/25 and very happy. “Thanks to a thorough exam, this patient was able to have surgery right away without being sent on a wild goose chase for unexplained vision loss,” Dr. Purman says.
“When patients come in with a remarkable health history, it is easy to be led down the wrong path and overlook the simplest causes, thinking something more complicated is the culprit,” Dr. Purman says. “This has often led to multiple unnecessary referrals to retina specialists, neuro-ophthalmologists and costly hospital visits for MRIs, all before seeing a cataract surgeon for the treatment they need.”
While it is necessary to find the cause of unexplained vision loss, it’s equally as important to take the entire exam into consideration before forming a diagnosis. Carefully examining the cornea, lens, macula and nerve when decreased vision occurs can help catch these changes before referring to another doctor.
Retina is a common first referral for these patients—to look for an occult macular change that is not seen on a dilated fundus exam. These patients will be given a clean bill of retinal health but may continue down the referral chain. When we don’t look for milky nuclear sclerosis, it will continue to hide right in front of us. “Any time a patient comes in with a large unilateral myopic shift that comes on suddenly, milky nuclear sclerosis is on my differential list,” says Dr. Purman.
An Integral Resource
The most common treatment for milky nuclear sclerosis patients is cataract surgery. Because this patient population tends to be younger, most still have accommodation left and would benefit from a discussion on monovision, toric lenses, multifocals, or a trifocal intraocular lens.
Educating your patients about these lens options beforehand is a great way to not only ensure a happy patient post-op but also positions you as the key information source for all things eye-related.
“In most cases, we have spent years with the patient and know their lifestyle goals, personality type and vision needs,” Dr. Purman says. “We should be an integral part of the decision process and refer to surgeons who will respect our wishes and whose skills will provide the best outcomes.”
