 |
The Optometric Retina Society refers to posterior segment care as “the new optometric frontier.” While that characterization is accurate in many ways, the fact is that optometrists have been examining, diagnosing and comanaging diseases of the retina for more than 100 years. The ability to manage these diseases was often preceded by the development of monitoring technology. Every step of the way, Review of Optometry has been there as a beacon to clinicians, shining its light on the innovations that would steer them faithfully toward the future.
Back in Time
Once researchers understood it was possible—using feline cadaver eyes—to visualize the fundus and the entrance of the optic nerve, engineers went to work designing an instrument with which to do so for the living eye.1 That’s when, in 1847, English mathematician Charlie Babbage presented “the model of an instrument … for the purpose of examining the interior of the living eye. It consisted of a small plane glass mirror from which a portion of the silvering had been removed.”1 Eventually, this instrument was independently redesigned by Hermann von Helmholtz to provide better illumination and the modern ophthalmoscope had its original ancestor.1
In 1915, Francis A. Welch and William Noah Allyn refined the ophthalmoscope even further by designing a hand-held, direct illuminating device. (On a side note, the company they started after this invention, Welch Allyn, still thrives as a manufacturer of a variety of medical devices).
From there, innovation snowballed and, with it, optometry’s understanding of several retina-based diseases. For instance, “it was soon discovered that many conditions of the blood, and the vessels, became manifest in the retina, through a change in the size and tortuosity of the vessels, and through the size and arrangement and location of a small area of inflammation or atrophy, which invariably followed such blood diseases as Uremia, Leukemia, Syphilis, Diabetes, and Albuminuria,” reads a 1933 issue of Review.2 In fact, the successors of the original ophthalmoscope would become useful in identifying systemic diseases such as arteriosclerosis (as was documented in a November 1940 issue of Review) and diabetes.3
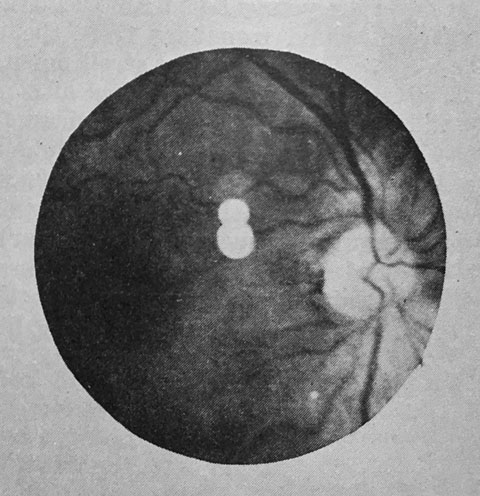 |
| The Optical Journal and Review of Optometry was one of the early venues to obtain education using images, such as this shot from a 1940 issue. However, the ability to reproduce these images in high quality, or even in color, was extremely limited. |
A New Wave
Fifty years after that, another big technological leap would redefine retina care: the development of fluorescein angiography (FA) for the eye. This technique—developed for diagnosis of ocular conditions in the 1960s—would go on to become the standard of care for imaging ocular circulation and the diagnosis of vascular disease. It is also of particular value in detecting and defining physiologic and anatomic changes in the fundus. So much of our understanding of retinal diseases was based on discoveries seen with FA. By giving us the ability to observe the fine meshwork of choroidal neovascularization (CNV), it became essential in the classification of retinal vein occlusions (ischemic vs. nonischemic) as well as helping to determine the extent and severity of diabetic retinopathy and other conditions.
The advancement of FA and the ability to diagnose diseases earlier led to treatments for many of the more common retinal diseases such as macular degeneration and diabetic retinopathy. The ability to distinguish CNV on FA led to a new classification system for CNV that became the basis for the macular photocoagulation study (MPS), which resulted in the first successful treatment for wet macular degeneration. As exciting as that time in eye care was, it was only the tip of the iceberg for things to come.
During that era, optometry gained significant ground in scope of practice laws. By the 1980s, ODs achieved parity with ophthalmologists in the ability to perform comprehensive eye exams, pupillary dilation and retinal examination with indirect ophthalmoscopy.
Let’s Get Digital
In a 1989 Review of Optometry issue focusing on the “tools of tomorrow,” Larry Alexander, OD, author of the highly-regarded Primary Care of the Posterior Segment, explained, “With today’s [that is—1989’s] instruments, it’s often difficult to detect small color shifts that herald vascular changes or edema […] soon, we will have a highly sophisticated, sensitive instrument that will help solve many of these concerns, an instrument called a digital imager.”4 He said this device will “integrate a camera and a computer to create, enhance, analyze and store three-dimensional pictures” as well as create a topographic map on the retinal surface, calculate the true color density of the area and enhance various aspects of the image, such as the brightness or contrast.4 He was right on the money as, today, digital cameras populate our exam lanes. These devices brought their own controversies. For instance, an April 1999 article pointed out that “retinal photos are not a substitute for a dilated fundus exam. A photo taken through an undilated pupil will not provide any information about the peripheral retina.”5 Today, the mainstream use of Optos widefield nonmydriatic fundus camera even challenges that tenet.
 |
| A 1999 article warned readers that a photo taken through an undilated pupil could not image the peripheral retina. |
As important as this technology is, its path to success wasn’t as smooth as you might expect. Considerable controversy surrounded how to use it in clinical practice and whether it could be a substitute for a dilated fundus exam. In June 2002, Review chronicled the launch of the Optomap Panoramic 200, which allowed a 200-degree field of view without pupillary dilation.6 Several ODs surveyed in the article raved about the quality of the imaging and the extent of the field of view. “We have found ourselves viewing areas of the retina the we oftentimes overlook with routine dilation” reported one OD. When asked if devices like that one could be a substitute for a dilated fundus exam, the consensus was “it does not: Anybody that tells you that is lying.”6
Today’s fundus imaging has evolved to smaller, more portable cameras with better nonmydriatic imaging, electronic illumination control, automated eye alignment and high-res digital image capture. They incorporate more patient-friendly light sources such as LEDs as well as laser scanning imaging. These improvements have helped make modern fundus photography a standard in almost every ophthalmic practice.
The Ease of Being Green
The innovation of digital cameras went hand in hand with another development from the 1990s—idocyanine green (ICG) angiography. Using this approach, traditionally associated with cardiovascular care, eye care professionals could pair the dye with the new, sensitive digital cameras for real-time visualization of the deeper vascular structures, enabling a better understanding of diseases that involve the choroid and retinal pigment epithelium. It was through ICG angiography that we learned that central serous is a choroidal disease that has secondary effects in the retina and RPE. In patients with posterior uveitis, ICG became an essential tool for the diagnosis and understanding of conditions such as multiple evanescent white dot syndrome (MEWDS) and multifocal choroiditis and panuveitis, which predominantly involve the choroid. Interesting, as important as ICG was, it never gained the kind of traction or had the impact of traditional fluorescein angiography, though it is still an important tool retinal specialists commonly use today.
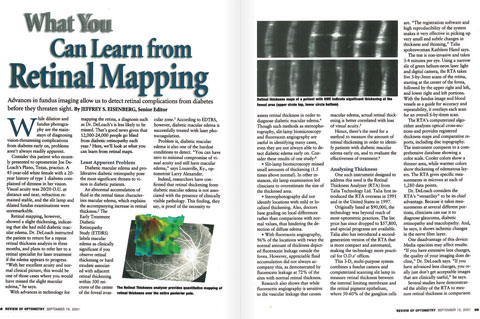 |
| This 2001 Review of Optometry article introduced readers to the many applications of optical coherence tomography. In retina care, imaging technology has always driven the OD’s ability to manage disease. |
OCT, Surprise!
In September 2001, Review featured a report titled “What You Can Learn from Retinal Mapping,” in which optical coherence tomography (OCT) was described as a technology that “works like a B-scan ultrasound to provide cross-sectional images of the retina […] allowing a 10µm to 20µm resolution.”7 The writers may not have known it at the time, but OCT would go on to be, perhaps, the most significant technological discovery in modern eye care. The article discussed OCT’s ability to detect diabetic macular edema (DME); in fact, “in some instances the OCT detected thickening when biomicrosopy did not.”7
In 15 years, the machines have only improved, upgrading from time-domain to spectral-domain OCT (SD-OCT), and a variety of offshoots. A 2009 article, “Get Familiar with SD-OCT,” offered an extensive tour of SD-OCT in which five cases demonstrate how SD-OCT can “illustrate retinal anatomy in better detail than clinical observation alone.”8
ODs Just Wanna Have Fundus Autofluorescence
Also emerging in the early 2000s, a new way to image the back of the eye became another essential tool for imaging macular disease. Fundus autofluorescence (FAF) uses the fluorescent properties of lipofuscin to study retinal disease in vivo.
FAF can be used to image macular degeneration, Stargardt’s disease, retinitis pigmentosa and central serous retinopathy. FAF was also a recommended modality for following patients on Plaquenil (Covis Pharmaceuticals).
In Review’s 2012 guide to retinal disease, Jeff Gerson, OD, provided a comprehensive review of FAF.9 His report states “not only can FAF be an ideal tool for documentation, but also it will often serve as a diagnostic modality because the device can elucidate many conditions that are invisible through traditional means of examination.”9
Dr. Gerson went on to say that “FAF can detetect structural abnormalities and predict functional defects.”9
The Future’s So Bright, I Gotta Wear Shades
Looking ahead, it seems adaptive optics may be among the next generation of imaging technologies—one that may provide even higher quality images than today’s OCT. By correcting for aberrations in the eye through improvements in lateral resolution, adaptive optics is able to achieve resolutions of about 2µm, high enough to identify even cone photoreceptors. This tool is still in its infancy and is limited to research use. It likely won’t be commercially available any time soon, but it represents another important evolutionary step in imaging.
In the last 125 years, ODs have seen some incredible advances with imaging innovations that are only picking up momentum as time goes on. Lucky for us, Review of Optometry has been there every step of the way.
|
1. Poser M. History of the Ophthalmoscope. Optical Journal-Review. 1941;78(2):106-18. 2. Breakthrough in diagnostic technology. Review of Optometry, 2011;148(8):55. 3. Tower P. Fundus changes in the arteriosclerosis. Optical Journal and Review of Optometry. 1940;21:20-23. 4. Alexander L. A new image for fundus evaluation. Review of Optometry. 1989;126(9):42-44. 5. Brooks R, Quinn C. How to get reimbursed for retinal photography. Review of Optometry. 1999;136(4):69-72. 6. Black A. Panoramic200: A new protocol for dilation. Review of Optometry. 2002;139(6);41-2. 7. Eisenberg J. What you can learn from retinal mapping. 2001;138(9):68-74. 8. Slotnick S, Sherman J. Get familiar with SD-OCT. Review of Optometry. 2009;146(6):79-85. 9. Gerson J. The clinical utility of fundus autofluorescence. Review of Optometry: 9th Annual Guide to Retinal Disease. 2012;149(4):S3-S5. |
