Because the eye is an extension of the brain, a neurologic examination can be a crucial diagnostic tool. The neuro exam allows you to assess structures neighboring those that are important to vision and can help determine the level of urgency for a patient’s ocular findings such as visual field defects, cranial neuropathies, double vision, optic neuropathy, ptosis, pupillary abnormalities and loss of vision. It may increase your clinical suspicion for underlying etiologies, including stroke, space-occupying lesion and demyelinating disease, among others.
Incorporating the neurologic exam into your tool box will help you provide exceptional care to your patients. Here we show you how and provide several case examples.
 |
| Fig. 1. Demonstration of upper extremity strength assessment. |
The Five-step Exam
As important as the neurologic exam is, it doesn’t take advanced technology to perform, and the tools are readily available in an optometric office. Clinicians can tackle the neurologic examination by breaking it into five sections:
1. Mental status. Many practitioners assess mental status at the beginning of the exam and, for healthy patents, write “A&Ox3,” representing Alert and Oriented to (1) person, (2) place and (3) time. If the patient is answering your questions inappropriately and seems confused or disoriented, you may choose to perform a mini mental status exam (MMSE). This questionnaire is designed to assess different aspects of cognitive function, including orientation, recall and language. The MMSE is quick and requires no training, although it may not detect mild cognitive decline.1
2. Cranial nerve testing. You will already have tested four of the 12 cranial nerves (CNs) during your routine eye exam: II, III, IV and VI. Before you tackle your first neurologic exam, we recommend you review the anatomical locations and pathways of the cranial nerves.
Cranial nerve testing can provide strong localizing data for a lesion. For example, if multiple cranial nerves are affected, the clinician can consider where cranial nerves share a common space, such as within the cavernous sinus (recall that CN III, IV, VI, the ophthalmic division of the trigeminal nerve, or V1, and the maxillary division of the trigeminal nerve, or V2, course here) or the superior orbital fissure (which contains CN III, IV, VI and the frontal, lacrimal and nasociliary branches of the trigeminal nerve). Table 1 reviews CN functions and outlines how to test for any dysfunction during a neurologic examination. Here is a brief review of the clinical applications of testing each cranial nerve:2
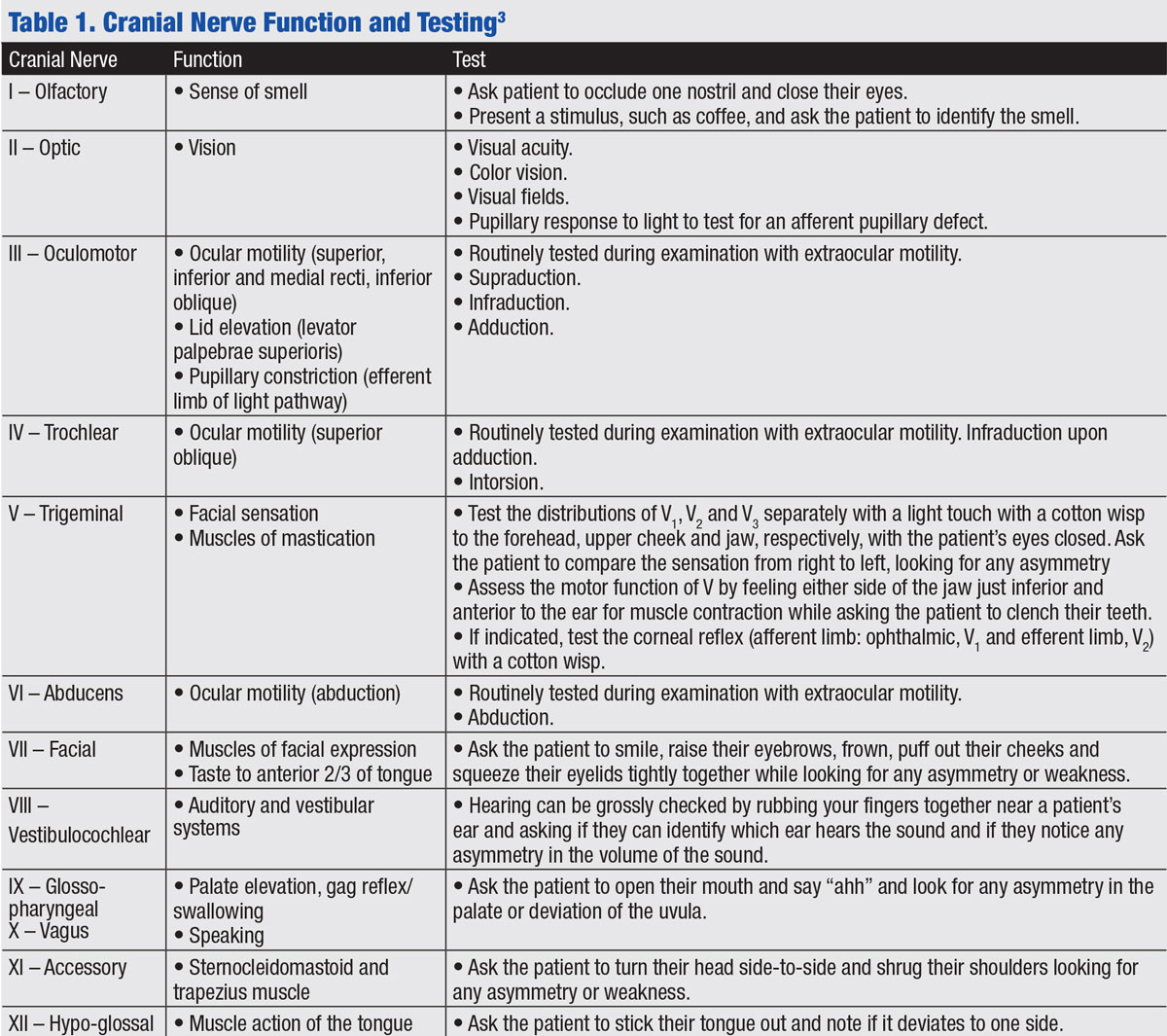 |
| Click table to enlarge. |
CN I: This nerve is often not tested unless a frontal tumor is suspected, such as in Foster-Kennedy syndrome, which is characterized by pallor of one optic nerve due to compression and edema of the contralateral nerve due to increased intracranial pressure.
CN II: This afferent nerve is assessed during visual acuity, color vision, pupil testing with the swinging flashlight test for afferent pupillary defect and visual field testing (see “Beyond Visual Field Testing”).
CN III: This is routinely tested with extraocular motility. It innervates the levator palpebrae superioris (elevation of the upper eyelid) as well as four of the six extraocular muscles and is involved in elevation, depression and adduction of the eye. It is also involved in pupillary constriction. A pupil-involved CN III palsy is more concerning for an aneurysm because pupillary fibers travel on the external surface of the nerve and are subject to compression
CN IV: This is also routinely tested with extraocular motility. It innervates the superior oblique muscle involved in depression of the adducted eye, as well as intorsion. Cover testing in multiple positions of gaze demonstrates a hyper deviation worse on contralateral gaze and ipsilateral head tilt.
CN V: Reduced sensation in the distributions of V1 and V2 may indicate a cavernous sinus lesion, especially in cases of CN III, IV and/or VI dysfunction.
CN VI: Routinely tested with extraocular motility, CN VI innervates the lateral rectus muscle which abducts the eye. Abduction deficits may be found in cases of increased intracranial pressure.
CN VII: This is a helpful test when you note facial asymmetry or an abduction deficit. An upper motor neuron lesion of CN VII (such as a stroke) will spare the forehead and indicates damage in the cerebrum. A lower motor neuron will affect the entire half of the face.
CN VIII: In a patient with an abduction deficit, it is important to test hearing due to the close relationship of cranial nerves VI, VII and VIII in the cerebellopontine angle. A patient with an abduction deficit and hearing loss on one side would localize to this region and would be concerning for a lesion such as an acoustic neuroma. Unilateral hearing loss is rarely due to a central lesion within the brain due to the extensive crossing of the auditory pathway.
CN VIII is also involved in the vestibular system, which is responsible for balance, proprioception and eye movements, including the vestibulo-ocular reflex. Disruption to this system can manifest clinically as nystagmus which may be seen in conditions such as Meniere’s disease.
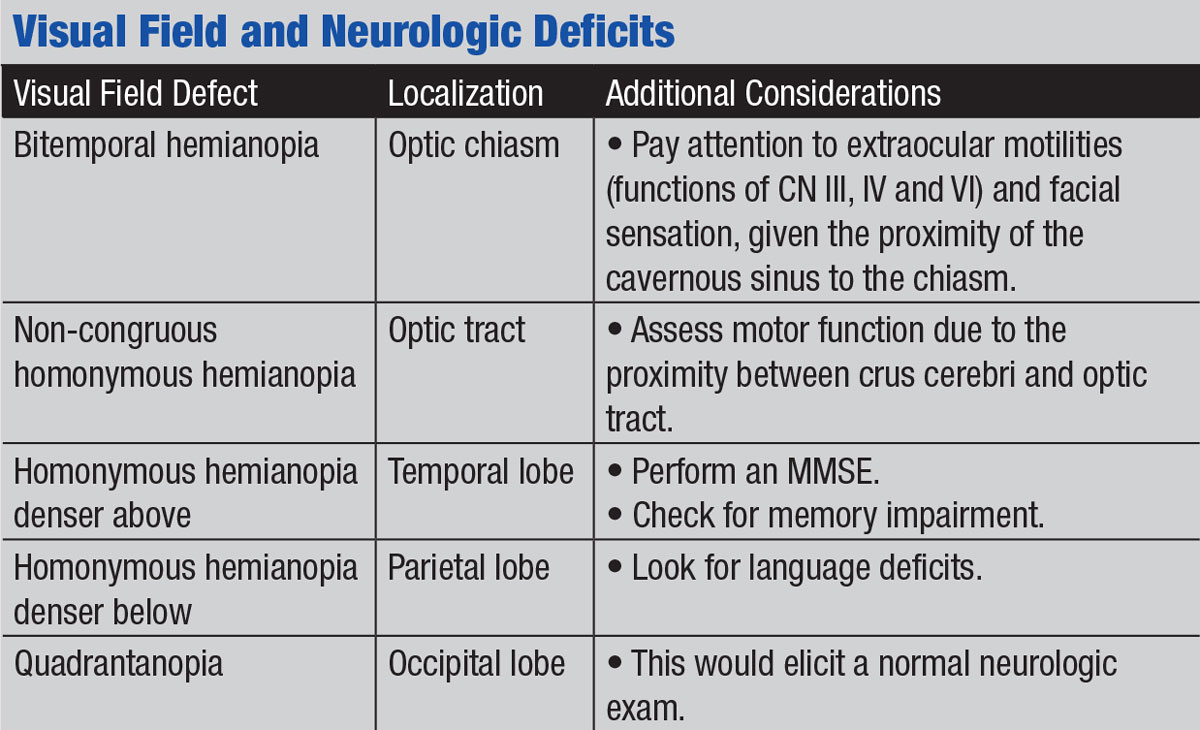
Beyond Visual Field TestingVisual field testing can unmask a number of associated neurologic conditions, given the expansive visual pathway. The anatomy of the visual pathway allows defects to be localized to anterior to the chiasm, the chiasm and posterior to the chiasm. If testing reveals a bitemporal hemianopsia, the lesion can be localized to the chiasm due to the anatomical crossing of the nasal retinal fibers. A pituitary adenoma is a common pathology that causes compression of the chiasm. In these cases, you must pay careful attention to extraocular motilities, as the cavernous sinus is adjacent to the sella. Recall CN III, IV, and VI course through the cavernous sinus and may be affected if there is lateral expansion of a sellar mass. In addition, by performing a neurologic exam you can assess the remaining cranial nerves within the cavernous sinus (CN V1 and V2). A homonymous hemianopia visual field defect suggests pathology posterior to the chiasm. Additional neurologic exam findings may help you to localize the lesion to the optic tract, parietal or temporal radiations, or the occipital lobe. For instance, should you detect weakness of the extremities on the same side as the patient’s hemianopia, consider an optic tract lesion. Anatomically, the optic tract runs adjacent to the crus cerebri, which carries the descending motor pathway in the midbrain. A lesion in this region is above the crossing of the motor pathway; therefore, weakness will be on the contralateral side. Thus, a patient with a right homonymous hemianopia and right-sided weakness may have a lesion affecting the left optic tract and left crus cerebri. Moving posterior, lesions of the optic radiations within the parietal and temporal lobes often have neurologic signs. A homonymous hemianopia denser above suggests pathology to the optic radiations that course through the temporal lobe; accompanying cognitive impairment may indicate the need for an MMSE. A homonymous hemianopia denser below accompanied by language deficits may suggest a lesion within the parietal lobe. Conversely, a visual field defect in the absence of other neurologic findings often localizes to the occipital lobe.1
|
CN IX and X: These are not examined separately; their close anatomic relationship rarely results in isolated lesions. Dysfunction of these nerves or the structures that they innervate may be indicated by dysphonia, dysphagia or dyspnea. Pay special attention to CN IX and X in patients with diplopia, ptosis or both, as they may be involved in myasthenia gravis, therefore raising clinical suspicion for disease of the neuromuscular junction.
CN XI: Upper motor neuron lesions will relatively spare the sternocleidomastoid muscle function and comparatively affect the trapezius muscle function more. This is also important to test in cases suspicious for myasthenia gravis.
CN XII: The tongue will deviate to the contralateral side of an upper motor neuron lesion and to the ipsilateral side with a lower motor neuron lesion. Tongue atrophy is a sign of a lower motor neuron lesion.
Cranial nerve testing clinical case. A poorly controlled diabetes patient presented with diplopia and an abduction deficit (75% of normal capability) concerning for a CN VI palsy. Neurologic examination revealed a subtle ipsilateral facial palsy that we could have easily missed with observation alone. All other testing of cranial nerve functions was normal. Despite the patient’s vasculopathic risk factor of poorly controlled diabetes, the concurrent CN VII palsy raised suspicion for an alternative etiology. Given the close association between cranial nerves VI and VII within the pons and as they exit the brainstem, simultaneous dysfunction suggests a lesion in that region. We referred the patient for additional testing, including an MRI of the brain, which resulted in the diagnosis of metastatic cancer and referral to oncology for further evaluation.
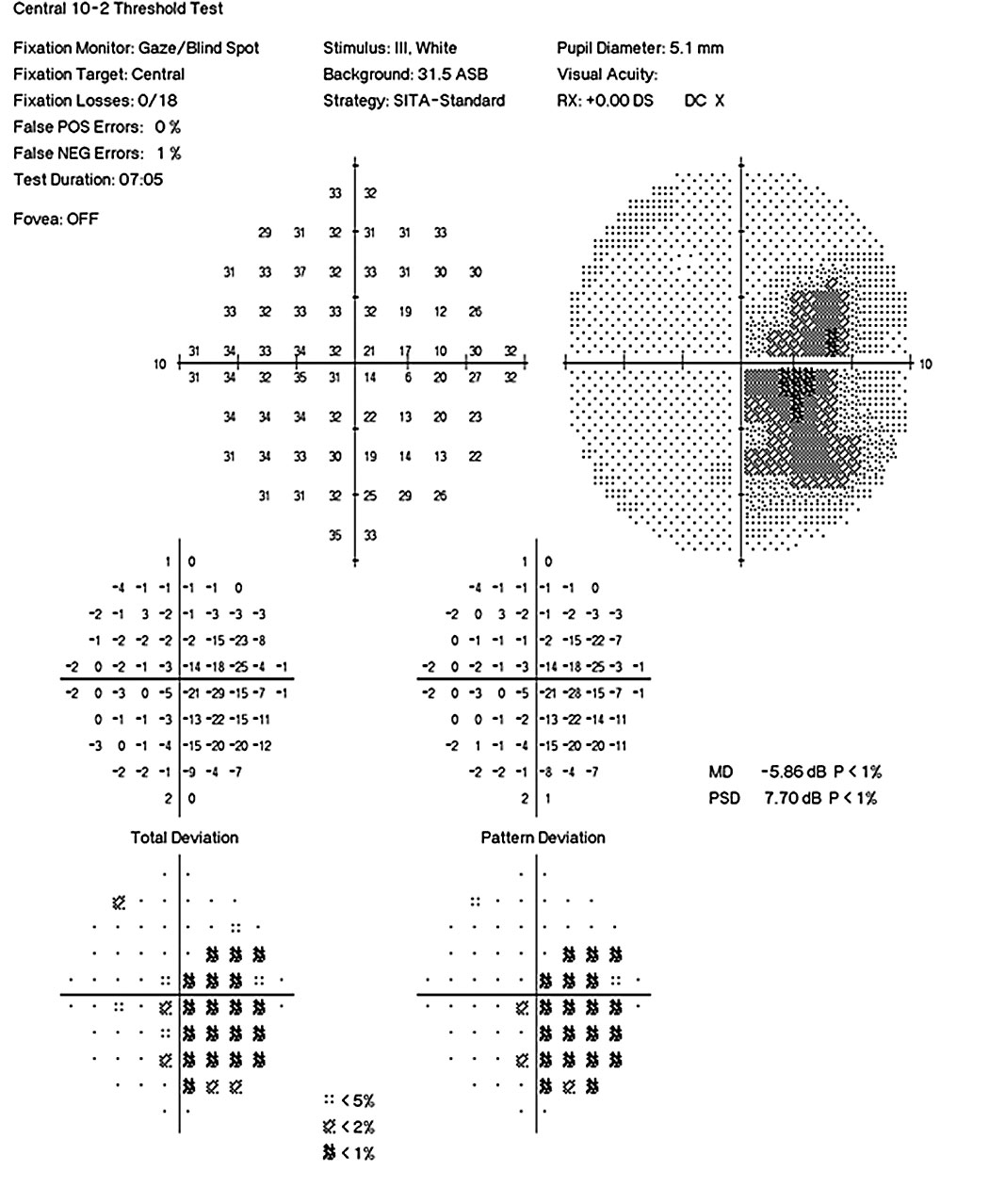 | 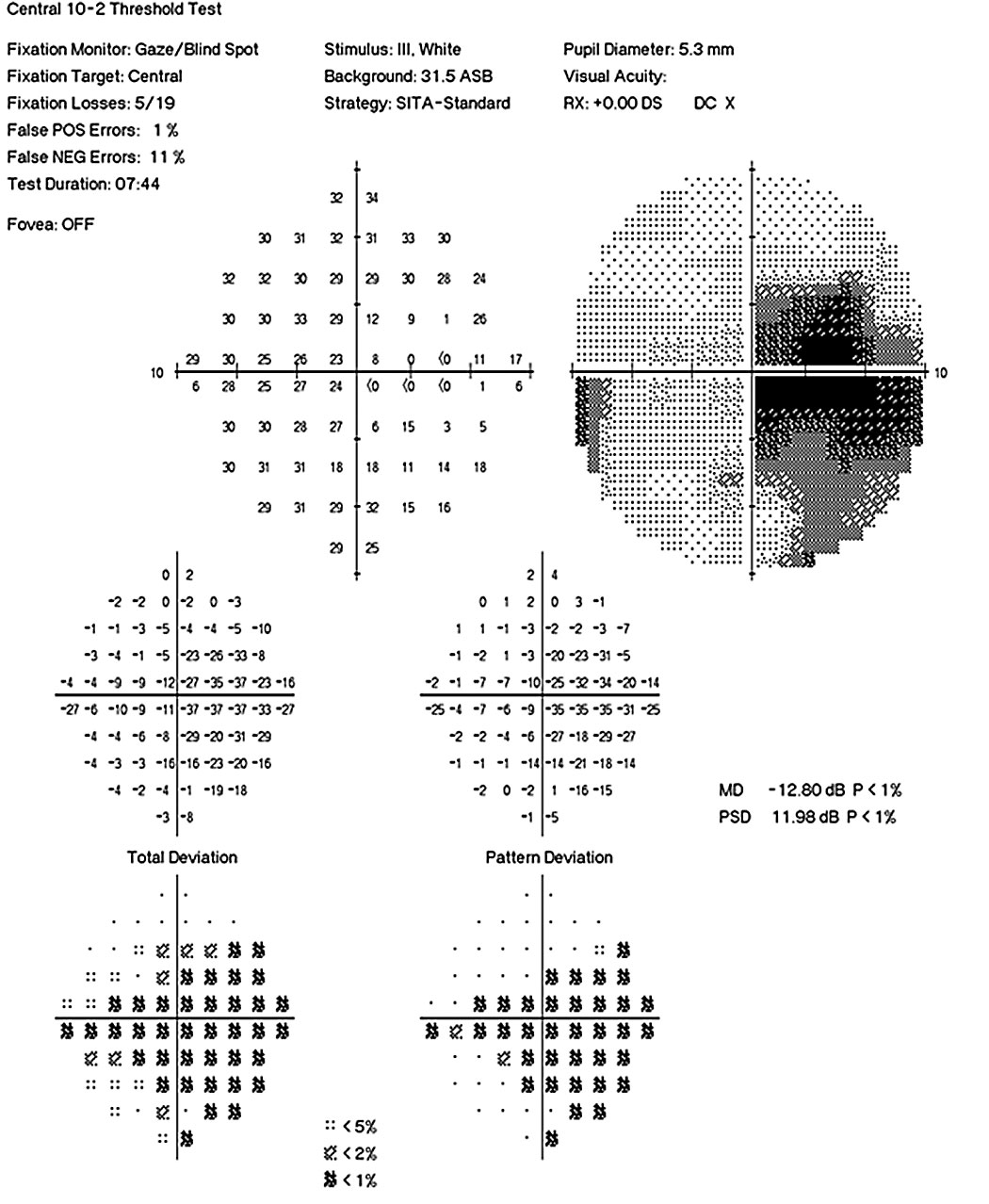 |
| Fig. 2. Humphrey 10-2 visual fields OS and OD show a more severe visual loss in the left eye compared with the right. | |
3. Motor/reflex examination. This begins with observation. You should first look for any involuntary movement such as tremors suggestive of basal ganglia disease (e.g, Parkinson’s) or muscle atrophy. Next, check for weakness of the upper and lower extremities by asking the patient to flex, extend, abduct and adduct their arms and legs against resistance. Compare the strength and ability of each muscle group with the contralateral side, looking for any asymmetry (Figure 1).
Weakness may be subtle and can be further elucidated with specific tasks. Ask a patient to hold both arms out in front of them with their palms facing upward and close their eyes. A slow, downward drift and pronation of one arm suggests weakness. Additionally, check fine movements by asking the patient to rapidly tap a finger or alternate their hand in a palm-up, palm-down fashion. Deep tendon reflexes may be diminished, such as in patients with Adie’s tonic pupil, or abnormally increased, such as in patients with multiple sclerosis.3
Motor/reflex examination case. A 66-year-old patient presented emergently with complaints of double vision. The patient had poorly controlled diabetes and blood pressure was elevated at the time of the exam. The patient denied any associated neurologic symptoms such as weakness, paresthesia or headache. Examination revealed a right abduction deficit concerning for a CN VI palsy, but the eye examination was otherwise normal. A neurologic exam revealed a previously unknown upper extremity, left-sided weakness. All other aspects of the neurologic exam were normal. An abduction deficit with contralateral weakness is concerning for a lesion in the brainstem, specifically referred to as Raymond’s syndrome. The patient was referred immediately to the hospital where neuroimaging revealed an infarction of the right ventral pons.
These first two cases discussed highlight the importance of performing a neurologic examination on patients with diplopia. The presence of additional neurologic symptoms (cranial neuropathy and weakness) that the patient may or may not be aware of should prompt you to pursue a more urgent work-up. If this patient had been evaluated from purely an ophthalmic standpoint, the CN VI palsy may have been presumed ischemic or vasculopathic, given the poor control of systemic disease. However, the discovery of a concurrent new-onset neurologic symptom raised significant concern and warranted immediate neuroimaging. While a cranial nerve palsy may be secondary to vasculopathic risk factors, it is important to consider that a diagnosis of exclusion.
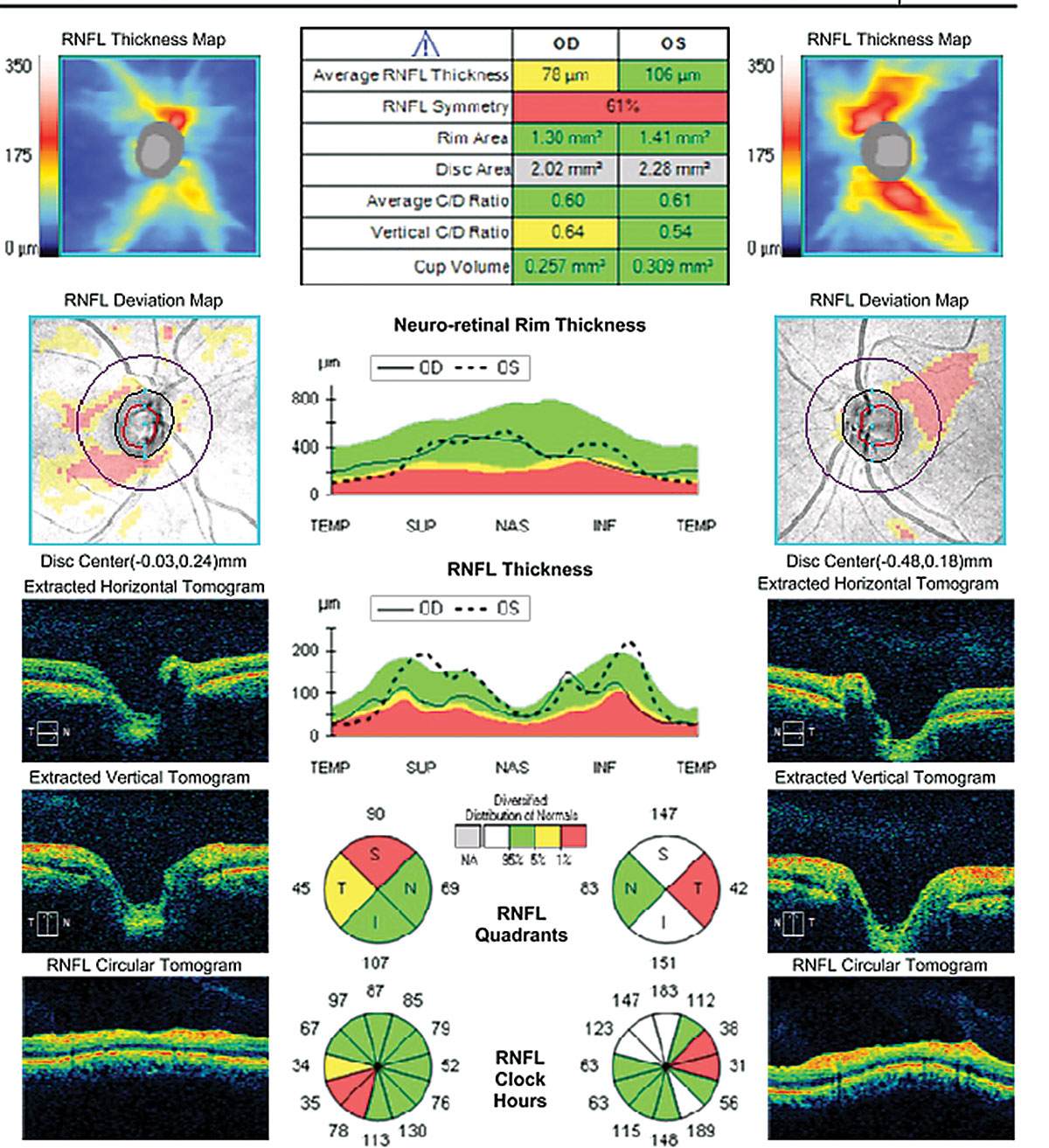 |
| Fig. 3. OCT of the optic nerves reveal temporal retinal nerve fiber layer thinning flagged on the deviation map. |
4. Coordination/gait. The first indication of cerebellar dysfunction may be observed as the patient walks to the exam room. Those with the condition may exhibit an ataxic, or clumsy, gait. You can also ask the patient to walk heel-to-toe in a straight line. Wheelchair-bound patients can slide their heel along their contralateral shin toward their foot. Inability to perform any of these tasks indicates potential cerebellar dysfunction or intoxication.
The presence or absence of ataxia may also be detected by asking the patient to quickly touch their finger from their nose to your fingertip an arm’s length away. Any hesitation, overshoot or undershoot, shaking or difficulty when they are about to touch your finger may indicate ataxia. Stand far enough away so that these patients have to fully extend their arm to reach your finger. You can move your finger to different areas to increase difficulty.
To assess rapid alternating movements, ask the patient to tap the palm of their hand on their leg repeatedly and quickly. Then ask them to flip their hand from palm to the back of the hand on their leg. Inability to do so is known as dysdiadokinesia and is often a sign of cerebellar disease, including stroke and atrophy.
The classic ocular manifestation of cerebellar dysfunction is nystagmus, with other potential ocular complications such as abnormal pursuits and optokinetic response. However, nystagmus is not only caused by cerebellar disease and can be due to vestibular dysfunction as well as other etiologies such as albinism and medication use (such as anti-seizure medications). Therefore, performing a neurologic exam on patients with nystagmus and paying special attention to their coordination and gait can help increase or decrease your clinical suspicion for a lesion within the cerebellum.
Coordination/gait case. A 31-year-old woman presented with complaints of glare and reduced vision. Her best-corrected visual acuity was 20/25- OD and 20/100 OS. She demonstrated a 0.3 log unit relevant afferent pupillary defect of the left eye and reduced color vision (12/14 Ishihara plates OD, 3/14 Ishihara plates OS) (Figures 2 and 3). Fundus examination revealed bilateral temporal pallor OS>OD (Figure 4). A neurologic exam revealed tandem gait ataxia and a positive Romberg test, suggestive of cerebellar dysfunction. She also demonstrated fine motor weakness affecting the left hand more than the right. Records of recent lab work demonstrated significant vitamin B12 and folate deficiencies, which supported a nutritional optic neuropathy diagnosis.
This case highlights how a neuro exam helps to refine your differential diagnosis of an optic neuropathy. Potential causes of bitemporal pallor include inflammatory, infectious, nutritional and toxic conditions. Anemia is a common early symptom of vitamin B12 deficiency, while neurologic symptoms are typically found later. Neurologic symptoms arise due to demyelination and can include cerebellar ataxia and limb weakness.4,5 In this case, our neurological findings helped narrow our differential and avoid additional tests such as laboratory testing and neuroimaging.
5. General sensory exam. Pain, temperature, proprioception, two-point touch, light touch, pressure and vibratory sense are all general sensations. The stimulus travels from the site of stimulation to the cerebral cortex. Depending on the sensation, the pathway decussates, or crosses, the midline in either the low medulla or spinal cord. Lesions below the decussation cause ipsilateral loss of sensation. In general, lesions within the brainstem or the brain cause contralateral loss of sensation.
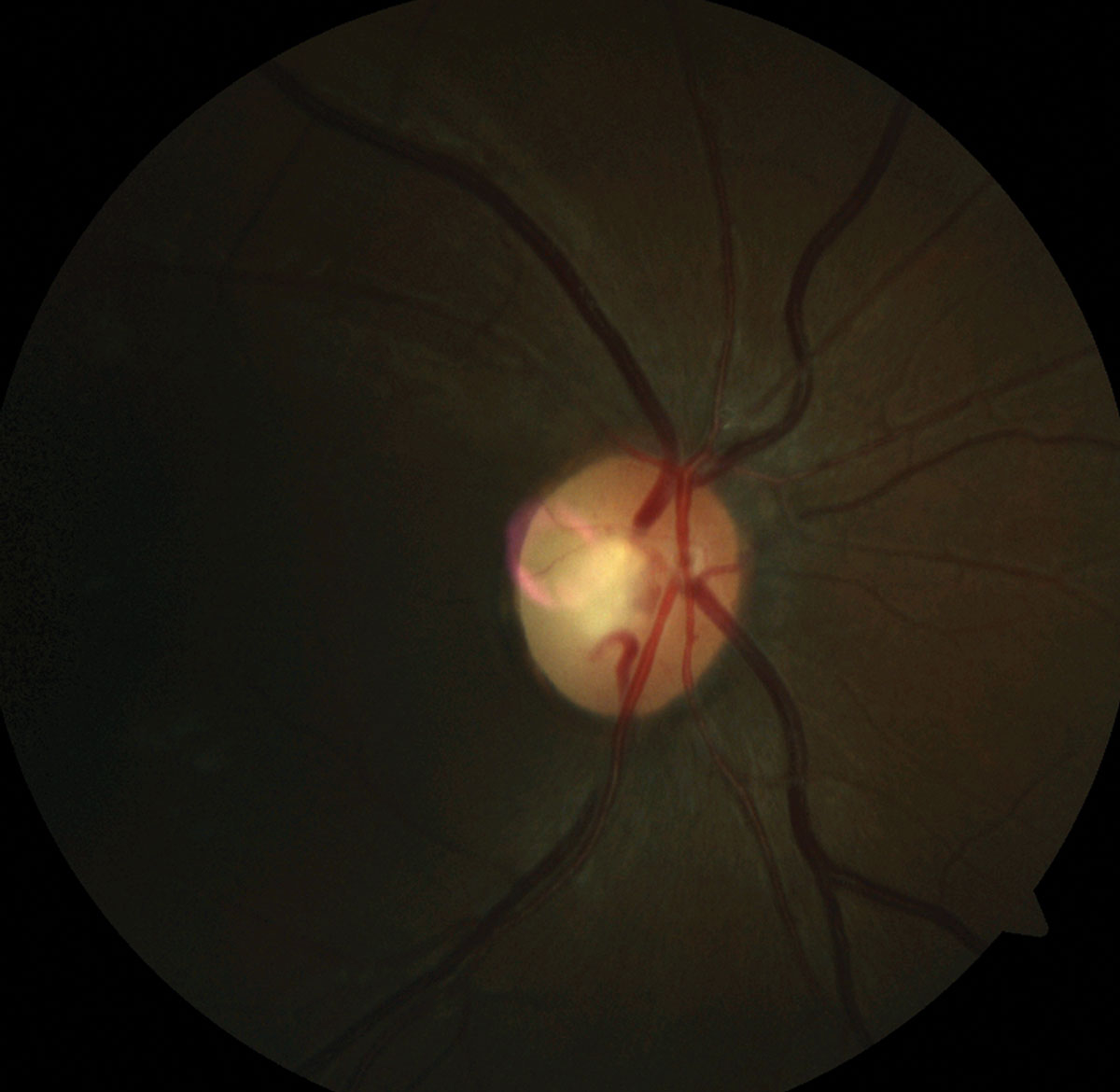 | 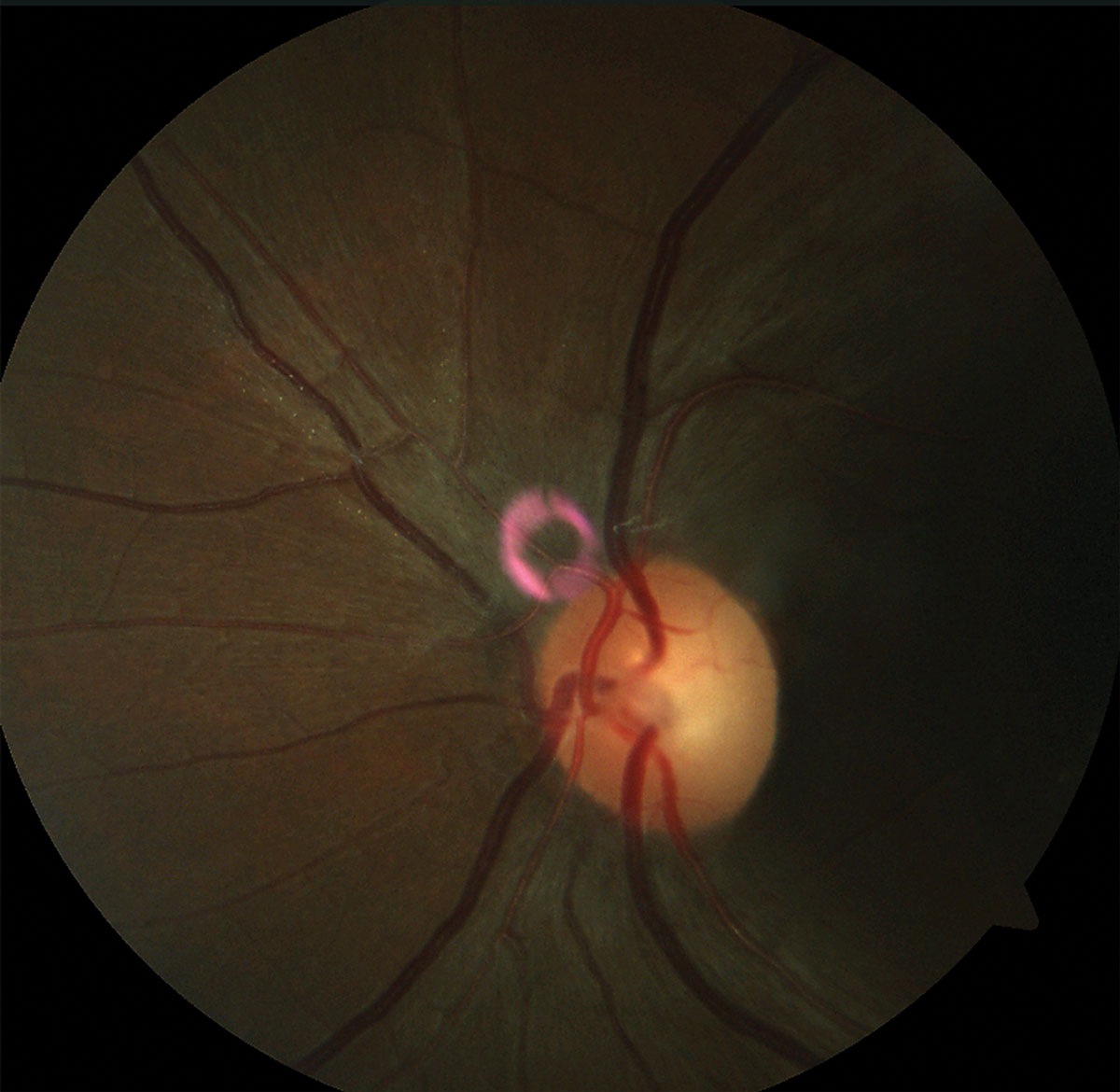 |
| Fig. 4. Note the pallor of the temporal rim in the patient’s fundus photo of the right optic disc and left optic disc (please disregard the pink artifact). | |
We recommend integrating tests of sensation with other elements of the neurologic exam. While the patient has their arms outstretched with closed eyes to test for pronator drift, lightly touch the backside of one of their hands and ask them to identify which hand was touched. Touch one hand, then the other and then both simultaneously while asking the patient to note any asymmetry. You may also touch a cool transilluminator on each of the patient’s arms to assess for asymmetry in temperature sensation.
Proprioception can be assessed by asking the patient to stand with their feet touching, known as the Romberg test. Patients can usually keep their balance with their eyes open due to visual cues; however, if they are unable to maintain their balance with their eyes closed—a positive test—they may have loss of proprioception. This test may also indicate cerebellar dysfunction.
Sensory exam case. A 62-year-old male presented with tearing affecting the left eye more than the right, a left-sided, non-congruous, homonymous hemianopia and intermittent diplopia. He reported a history of a hemorrhagic stroke affecting the right side of his brainstem. Neuro exam revealed left-sided weakness of the left upper and lower extremities. He also demonstrated notable sensory defects and a left-sided facial palsy that was not grossly evident by observation alone. By correlating our findings with the anatomical location of the stroke, we attributed his presentation to the prior stroke of the right pons, therefore avoiding any further testing or work-up. His previous MRI report was remarkable for gliosis involving the right optic tract, which corresponded with his visual field defect.
These cases highlight many important clinical implications of the neurologic exam, hopefully inspiring you to incorporate it into your practitioner’s toolbox. Ultimately, a neurology consult is often indicated, but an in-office screening may help narrow a list of differentials to help develop a sense of urgency. With practice, the neurologic exam can be performed and interpreted quickly and efficiently, with significant implication for patient care.
Dr. Maglione is an assistant professor at the Pennsylvania College of Optometry at Salus University and clinical instructor in the primary care and neuro-ophthalmic disease services at The Eye Institute.
Dr. Seidler graduated from the Pennsylvania College of Optometry at Salus University. She is currently completing a two-year advanced residency program at The Eye Institute in neuro-ophthalmic disease.
|
1. O’Bryant SE, Humphreys JD, Smith GE, et al. Detecting dementia with the mini-mental state examination (MMSE) in highly educated individuals. Arch Neurol. 2008;65(7):963-7. 2. Finsterer J, Grisold W. Disorders of the lower cranial nerves. J Neurosciences in Rural Practice. 2015;6(3):377-91. 3. Campbell W. DeJong’s The Neurologic Examination. 7th ed. Philadelphia: Wolters Kluwer; 2015. 4. Ralapanawa DMPUK, Jayawickreme KP, Ekanayake EMM, Jayalath WATA. B12 deficiency with neurological manifestations in the absence of anaemia. BMC Research Notes. 2015;8:458. 5. Ashizawa T, Xia G. Ataxia. Continuum: Lifelong Learning in Neurology. 2016;22(4):1208-26. |
