Dry eye disease (DED) is a common ocular surface condition with multiple and sometimes overlapping etiologies.1-4 When the disease becomes severe, it can cause major disruptions in a patient’s quality of life. Fortunately, they need look no further than their optometrist to bring these symptoms under control and get back to reading, driving and sleeping comfortably.
Even for patients with a severe case, the optometrist can take a lead role in identifying the underlying etiology and use a multifactorial approach to manage this disease state and its associated symptoms.
Identify the Etiology
Severe dry eye is often catalyzed by a primary etiology.2 That primary etiology is frequently inflammatory based and is either systemic (e.g., Sjögren’s, sarcoidosis, graft-vs.-host disease), or it is due to direct, localized inflammation of the patient’s ocular surface structures.2-9
However, researchers are also studying the corneal nerve as a potential instigator of severe dry eye.5-8 The densely innervated pain receptors in the cornea can respond to mechanical, chemical or temperature stimuli. These nociceptor terminals transmit signals along a complex neurological pathway, and the perception of pain can be:
(a) due to true exposure of the nerve endings;
(b) influenced by neural injury from chronic diseases that affect the density, size and tortuosity, and;
(c) a function of the nerves, or even representative of a central nervous system dysfunction.10-14
Although the role of these corneal nerves is complex, understanding it may help ODs manage DED.10-14
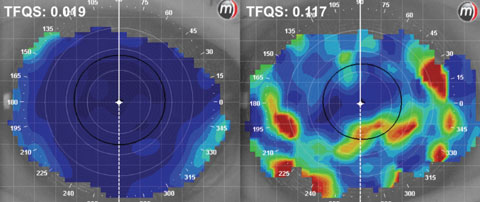 |
| Fig. 1. Tear film quality scores (TFQS) as measured by placido disc topography. A low score (left) indicates better tear film quality than a higher score (right). Click image to enlarge. |
Diagnosis and Management
Severity of dry eye can be measured subjectively, through the assessment of patient comfort and visual quality, and also using diagnostic techniques such as tear break-up time (TBUT), surface staining and meibomian gland patency. One of the challenges of dry eye diagnostics is that the severity is often mismatched between the subjective and objective modes of evaluation.9 While clinicians may see a disparity between objective and subjective tests, they only need one positive outcome to begin treating aggressively.
If the patient is reporting drastic reduction in their quality of life or, conversely, if their ocular surface appears to be at high risk for long-term damage, a diagnosis of severe dry eye is warranted.
Subjective severity is best quantified using a validated ocular surface disease survey, such as the Ocular Surface Disease Index (OSDI).10 After subjective testing, the ocular surface can be evaluated to determine the objective severity and, ultimately, the most effective approach to managing the patient.
When objectively evaluating the severity of dry eye, clinicians should carefully evaluate and grade each component of the ocular surface system to help direct their treatment. But they must also identify and capitalize on any features of the system that may be able to promote rehabilitation of the ocular surface and reduce symptoms of the condition. Here are the ocular surface systems that may be affected in the disease, the various methods of diagnostic evaluation and the acute and chronic treatment strategies for each component.
Meibomian Glands
Diagnostics: Clinicians should evaluate the MG comprehensively, from the orifice to the glandular structure. The orifices are best evaluated without stain (for capping and for lid margin telengectasias) and then with lissamine green (for devitalization and keratinization of the MG opening). The integrity of the glands themselves can be imaged using quantitative meibomography, which also allows quantitative monitoring over time. Commercially available diagnostic systems can image the area of the gland using infrared light and allow clinicians to observe the length, width and tortuosity of the glands (Figure 1). The images are grades from one to six to measure the level of MG atrophy.
Treatment and management: The first step to maximize treatment efficacy in patients with an MG deficient component to their dry eye is to use a cotton-tipped applicator or spud to debride devitalized cells and coagulated meibum from the MG orifices, which research shows, improves symptoms and MG function.11 For this technique, anesthesia isn’t necessary, and clinicians should use gentle motion and pressure of the spud to avoid debridement of healthy underlying tissue.11 Once the MG opening is visible, gland expression can be done manually or using advanced thermodynamic treatment systems (e.g., Lipiflow, TearScience; MiBoFlow, MiBo Medical). For patients whose glands have atrophied—which they often do in severe cases of dry eye—thermo-treatment is controversial.12 However, some experts believe these systems can be helpful even when there is extensive gland atrophy. Regardless, it is important to consider the atrophic state of the glands when deciding on treatment and to understand that the success of these systems may be limited by the stage of meibomian gland atrophy. Clinicians should focus on appropriate supplementation of the lipid layer if they’re unable to salvage the health of the glands (i.e., preservative-free artificial tears). When successful, repeated thermo-treatments every six to 12 months may be necessary to maintain meibum flow.12
For severe dry eye, low dose antibiotics and steroids are often necessary to acutely reduce inflammation and enhance potential recovery of the glands (Table 1). They are also often used to manage dryness. Lid hygiene and maintenance gland expression treatments should be recommended as needed; dietary supplementation (omega-3) may help reduce inflammation.8
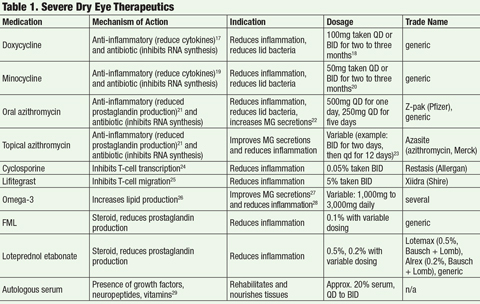 |
| Click table to enlarge. |
Tear Film
Diagnostics: To evaluate the status of the tear film itself, apply sodium fluorescein (NaFl) to the ocular surface to measure the TBUT. Additionally, advancements in corneal topography instruments now allow clinicians to evaluate the tear film non-invasively (without the use of NaFl, which disrupts the natural tear layer), and obtain sensitive objective data about the tear film through programs that measure its quality using placido disc technology. In addition, other instruments, such as the LipiView, offer a quantitative measure of tear film, and, specifically, lipid layer thickness. If available, using these systems prior to NaFl application will allow for a sensitive evaluation of tear characteristics that can be objectively monitored.
Whether non-invasive testing is available or not, NaFl should be applied to further evaluate the tear stability on the ocular surface, and assess the efficiency and apposition of the puncta.
Osmolarity testing, which is commonly performed in research, has become an essential modern diagnostic technique. It is a strong tool to asses the severity of dry eye, and has been shown to be more predictive of severity of the disease than several other tests, including MG grading, OSDI index, TBUT and staining.23 The published osmolarity threshold scores for grading severity of DED are variable, but an approximate threshold for severe dry eye is 320mOsm/mL.24 While this testing can be quite helpful, it is important to consider the effect of reflex tearing (diluting the tears and artificially lowering the osmolarity), and also on the diurnal fluxuations in osmolarity, which vary on average by approximately 20mOsm/L in dry eye patients.24 Measurement of inflammatory components in the tear film is also becoming a target for diagnostic technology.
Treatment and management: Replenishing the surface tear film with preservative-free artificial tears (PFAT) is always a part of dry eye treatment, continuous instillation of often indicated in severe dry eye patients. These not only act to supplement the natural tear film, but can also dilute the tear film and reduce the osmolarity, which can precipitate ocular surface damage.
Excessive tear drainage can be reduced by punctal occlusion with either plugs or cauterization. Remember to carefully evaluate the tears and ocular surface of a severe dry eye patient before recommending this treatment, and confirm the likelihood that the severe dry eye is exacerbated by excessive tear drainage. If the drainage system is not contributory to the severe dryness, punctal occlusion may do more harm than good. For example, if excessive inflammatory mediators are seen on the ocular surface, it would be more effective to mitigate those mediators using therapeutic intervention than potentially create stagnation on the ocular surface.
The Corneal Epithelium and Conjunctiva
Diagnostics: Ocular surface staining with NaFl is the traditional approach to evaluate the integrity of the cornea and conjunctiva. NaFl will stain irregularities in tear film apposition, but lissamine green should also be used in dry eye patients to specifically stain dead or devitalized cells on the ocular surface. Additionally, confocal microscopy can help evaluate the anterior cornea at the cellular level. Although the most severe involvement of the cornea in dry eye patients occurs at the level of the epithelium, the evaluation of epithelium via confocal microscopy is less validated than the more commonly used stromal evaluation. While the confocal microscopy technique is relatively novel in clinical practice, it is becoming more readily used in research and some clinical settings.
Treatment and management: To regenerate the epithelium in patients with severe dry eye, autologous serum is often part of the treatment regimen. In the most severe cases, an amniotic membrane should be applied prior to autologous serum implementation to give the surface a strong boost of growth factors and nutrients prior to the chronic treatment plan (Figure 2). Patients with severe dry eye often have severe, consistent breakdown of the ocular surface, so chronic treatments such as autologous serum and anti-inflammatory drugs are necessary. Scleral contact lenses have also become strongly indicated to protect the surface from environmental insult, which prevents a cycle of tissue stress, or further tissue breakdown that worsens the disease.
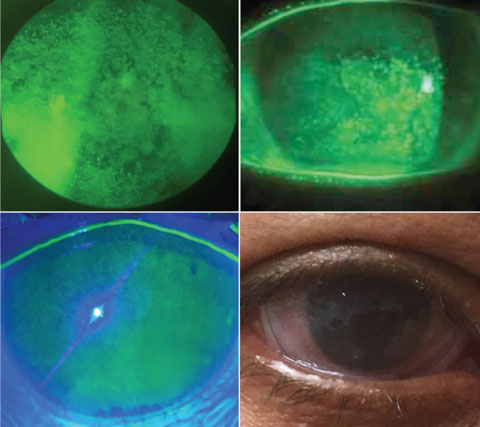 |
| Fig. 2. These epithelial staining examples all merit the use of an amniotic membrane (bottom right). Photos: Amber Gaume-Giannoni, OD, and Sheila Morrison, OD. Click image to enlarge. |
Inflammatory Mediators in the Tear Film and Ocular Tissues
Diagnostics: Some patients will exhibit classic and strong signs of clinical inflammation (redness, edema), which can be evaluated using a slit lamp; however, clinicians do not generally test for subtle up-regulation of inflammatory mediators that may contribute to the dry eye inflammatory state.
The most specific and clinic-friendly diagnostic test for measuring inflammation is the Inflammadry (Rapid Pathogen Screening), which measures the level of matrix metalloproteinase (MMP-9) in the tear film. Values greater than 40ng/ml will show a positive result (indicating increased inflammation).25
Treatment and management: In patients with severe dry eye, a therapeutic eyedrop that specifically targets inflammation should be prescribed, and many of the modern therapeutics for severe dry eye are centered on targeting inflammatory mediators on the ocular surface. Restasis (cyclosporine, Allergan) and Xiidra (lifitegrast, Shire) are two of the most common therapeutics, both developed to target T-cell activity and subsequent cytokine production. Cyclosporine interferes with T-cell transcription, and lifitegrast inhibits an integral protein complex (LFA-1/ICAM-1) that allows for T-cell migration.19,26
Autologous serum is also an appropriate adjunctive choice to target inflammation on the ocular surface, and there is potential for additional anti-inflammatory serum-derived treatments, as well as targeted mediation of inflammatory cytokine interleukin-1.27-29
Corneal Nerves
Diagnostics: Few advanced diagnostic techniques are available for evaluating the corneal nerves. Esthesiometry can quantify the level of pain, and help to locate any focal areas of extreme corneal sensitivity, and confocal microscopy is available to evaluate the cornea on a cellular level and allow visualization of the density, length and tortuosity of the corneal nerves.30
Treatment and management: Autologous serum drops contain several pro-epithelial and neural growth factors and are the strongest therapy recommended for corneal pain due to damage to the corneal nerve terminals.29 If the corneal pain is associated with dysfunction at a higher cognitive level than the peripheral nerve terminals, further neural evaluation may be needed to elicit the exact cause.
Scleral Lenses
Scleral lens treatment for dry eye can be extremely beneficial for patients, the primary advantage being that they cover and protect the anterior ocular surface (Figure 3). However, it is important to remember that scleral lenses are not intended to be a standalone treatment for dry eye. They are devices indicated for severe dry eye patients, and should be used as part of the treatment regimen to heal and protect the ocular surface while the adjunctive therapies can treat the targeted molecular level.
Large-diameter scleral lenses (>18mm) may be the most appropriate to use when treating DED due to their more complete coverage of the ocular surface, especially if the clinical signs show damage that extends far beyond the limbus on the conjunctiva. One of the benefits of these lenses is that they offer the opportunity to deliver co-therapies to the cornea, since preservative-free medications can be put into the bowl of the scleral lens prior to application for prolonged apposition to the ocular surface. Sterile saline is the most common application solution used with scleral lenses, although individuals with DED may benefit from the use of a non-preserved artificial tear. In addition, these patients could be prescribed off-label formations, depending on what preservative-free systems works best for each individual disease state.
The following are two agents to consider using in an application solution for patients:
1. Autologous serum drops (one vial per lens, or split a vial between each).
2. Preservative-free artificial tears (to top off the autologous serum drop, or exclusively).
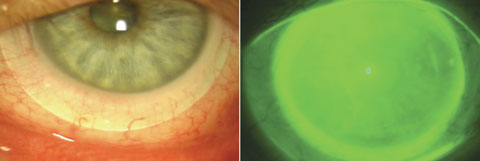 |
| Fig. 3. At left, a scleral lens allows full coverage of the cornea and variable conjunctival coverage with a 100µm to 200µm tear layer between the lens and the corneal surface. At right, the same eye with NaFl instilled to visualize the tear layer. Click image to enlarge. |
Patient Education
Optometrists should offer patients solutions for ocular surface disease that also promote the greatest quality of life and least inconvenience, as possible. While major advancements in the therapeutics and medical devices available for dry eye exist, a truly multifactorial approach to management of severe dry eye must be the standard of care. In severe cases, one of the most important aspects of treatment is education. The primary educational topics are:
1. The multifactorial and individualized treatment strategies, and the importance of careful compliance to each regimen.
2. The effect of exposure to elements (wind, dust, sun), and the effects of digital device fatigue and other external lifestyle influences.
3. The role of nutrition (e.g., omega-3 and omega-6 imbalance), hormones and overall systemic health (e.g., autoimmune diseases) in the success of their dry eye treatment.31
DED management has become an increasingly important role for the optometrist, especially as more information about the specific etiologies of the disease and the mediators involved come to light. As awareness grows, it is important to specifically identify etiologies and risk factors on a personalized level and customize our treatment plans.
Dr. Walker is an attending clinician at University of Houston College of Optometry.
|
1. Foulks GN. The correlation between the tear film lipid layer and dry eye disease. Surv Ophthalmol. 2007;52(4):369-374. 2. Stern ME, Pflugfelder SC. Inflammation in dry eye. Ocul Surf. 2004;2(2):124-30. 3. Calonge M, Enríquez-de-Salamanca A, Diebold Y, et al. Dry eye disease as an inflammatory disorder. Ocul Immunol Inflamm. 2010;18(4):244-53. 4. Baudouin C. The pathology of dry eye. Surv Ophthalmol. 2001 Mar;45 Suppl 2:S211-20. 5. Müller LJ, Marfurt CF, Kruse F, Tervo TMT. Corneal nerves: structure, contents and function. Exp Eye Res. 2003;76(5):521-42. 6. Hosal B, Ornek N, Zilelioglu G, Elhan A. Morphology of corneal nerves and corneal sensation in dry eye: a preliminary study. Eye (Lond). 2005;19(12):1276-9. 7. Rosenthal P, Baran I, Jacobs D. Corneal pain without stain: is it real? Ocul Surf. 2009;7(1):28-40. 8. He J, Bazan H. Omega-3 fatty acids in dry eye and corneal nerve regeneration after refractive surgery. Prostaglandins Leukot Essent Fat Acids. 2010;82(4-6):319-25. 9. Nichols K, Nichols J, Mitchell G. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004;23(8):762-70. 10. Hamrah P, Qazi Y, Hurwitz S. Impact of corneal pain on quality of life (QoL): The Ocular Pain Assessment Survey (OPAS) study. 2014;55(13):1469. 11. Korb D, Blackie C. Debridement-scaling: a new procedure that increases Meibomian gland function and reduces dry eye symptoms. Cornea. 2013;32(12):1554-7. 12. Blackie C, Carlson A, Korb D. Treatment for meibomian gland dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation. Curr Opin Ophthalmol. 2015;26(4):306-13. 13. Di Caprio R, Lembo S, Di Costanzo L, et al. Anti-inflammatory properties of low and high doxycycline doses: An in vitro study. Mediators Inflamm. 2015;2015. 14. Doughty MJ. On the prescribing of oral doxycycline or minocycline by UK optometrists as part of management of chronic Meibomian Gland Dysfunction (MGD). Contact Lens Anterior Eye. 2016;39(1):2-8. 15. Amsden G. Anti-inflammatory effects of macrolides-An underappreciated benefit in the treatment of community-acquired respiratory tract infections and chronic inflammatory pulmonary conditions? J Antimicrob Chemother. 2005;55(1):10-21. 16. Liu Y, Kam W, Ding J, Sullivan D. Can tetracycline antibiotics duplicate the ability of azithromycin to stimulate human meibomian gland epithelial cell differentiation? Cornea. 2015;34(3):342-6. 17. Luchs J. Efficacy of topical azithromycin ophthalmic solution 1% in the treatment of posterior blepharitis. Adv Ther. 2008;25:858-70. 18. Fan W, Liao H, Lai N. Topical cyclosporine therapy for keratoconjunctivitis sicca in Sjogrens’ syndrome. Tzu Chi Med J. 2003;15(2):85. 19. Perez V, Pflugfelder S, Zhang S, et al. Lifitegrast, a novel integrin antagonist for treatment of dry eye disease. Ocul Surf. 2016;14(2):207-15. 20. Liu Y, Kam W, Sullivan D. Influence of omega 3 and 6 fatty acids on human meibomian gland epithelial cells. Cornea. 2016;35(8):1122-6. 21. Rosenberg ES, Asbell PA. Essential fatty acids in the treatment of dry eye. Ocul Surf. 2010;8(1):18-28. 22. Goyal S, Hamrah P. Understanding neuropathic corneal pain—gaps and current therapeutic approaches. Semin Ophthalmol. 2016;31(1-2):59-70. 23. Potvin R, Makari S, Rapuano CJ. Tear film osmolarity and dry eye disease: a review of the literature. Clin Ophthalmol. 2015;9:2039-47. 24. Li M, Du C, Zhu D, et al. Daytime variations of tear osmolarity and tear meniscus volume. Eye Contact Lens. 2012;38(5):282-7. 25. Kaufman H. The practical detection of MMP-9 diagnoses ocular surface disease and may help prevent its complications. Cornea. 2013;32(2):211-6. 26. Paton DM. Lifitegrast: first LFA-1/ICAM-1 antagonist for treatment of dry eye disease. Drugs of Today. 2016;52(9):485. 27. Anitua E, Muruzabal F, de la Fuente. PRGF exerts more potent proliferative and anti-inflammatory effects than autologous serum on a cell culture inflammatory model. Exp Eye Res. 2016;151:115-121. 28. McKay T, Karamichos D. Quercetin and the ocular surface: What we know and where we are going. Exp Biol Med. 2017;246(6):565-72. 29. Fabiani C, Sota J, Tosi G, et al. The emerging role of interleukin (IL)-1 in the pathogenesis and treatment of inflammatory and degenerative eye diseases. Clin Rheumatol. Dec 28 2016. [Epub]. 30. Mantopoulos D, Cruzat A, Hamrah P. In vivo imaging of corneal inflammation: new tools for clinical practice and research. Semin Ophthalmol. 2010;25(5-6):178-85. 31. Miljanovic B, Trivedi K, Dana M. Relation between dietary n-3 and n-6 fatty acids and clinically diagnosed dry eye syndrome in women. Am J Clin Nutr. 2005;82(4):887-93. |
