While some enjoy the blooming flora and warm sun of spring, others only see elevated pollen levels and a rise in temperature as the dreaded start of allergy season. Their noses will stuff, their throats will itch and their eyes will become itchy and red. Sadly, many patients mismanage ocular allergy by employing over-the-counter (OTC) red eye solutions that neither address the problem nor relieve the symptoms. When it becomes too much, many of these patients will land in our offices seeking relief.
The good news is that allergy medication is more targeted than ever, and with the right background optometrists can bring patients the relief they’re seeking. Gone are the days when ODs simply threw a combination antihistamine and mast-cell stabilizer drop at anything that itches.
Over the last decade, an explosion of research has focused on the ocular surface, increasing our understanding of how our environment, and its offending allergens, impacts the anterior segment.
This article provides an update on the state of ocular allergy therapies and how optometrists can use that knowledge to bolster their roles in treatment.
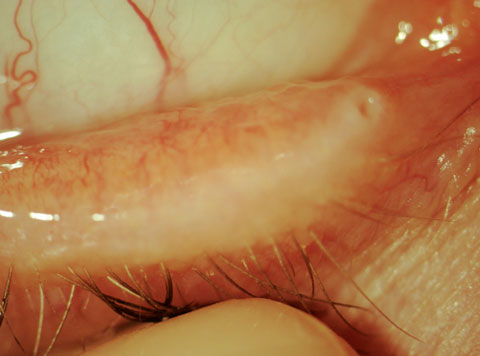 |
| This patient displays nasal inferior papillary conjunctivitis in the right eye. Click image to enlarge. |
Comorbidities
Before delving into ocular allergy management, get familiar with your comorbidities. In many cases, managing them can reduce the need for directly treating the allergic reaction. Some of my most successful cases have started with first managing the coexisting conditions that were exacerbating the allergy.
Demodex: Ask if the patient’s itch is directed toward the conjunctiva or the eyelid. If it’s the former, it’s likely the result of an allergy; if it’s the latter, you should suspect Demodex.1 Look closely at the base of the lash follicles for protruding tails. If you’re still unsure, try using forceps to gently twirl a lash within its follicle to draw out the mite.2 Patients with Demodex blepharitis alone will find no relief from topical allergy medications, so eradicating the mites via mechanical debridement and chemical eradication (e.g., ophthalmic-grade tea tree oil or hypocholorous acid 0.01%) is necessary to relieve itchy eyelids.3
Both patients suffering from allergy and Demodex should be advised to wash their linens weekly and to replace makeup containers to reduce exposure to offending agents. If patients are compliant with your Demodex treatment regimen and a papillary reaction is still present after several weeks (the life cycle of Demodex mites is approximately 14 days) adjunctive topical allergy medications are indicated.4
 |
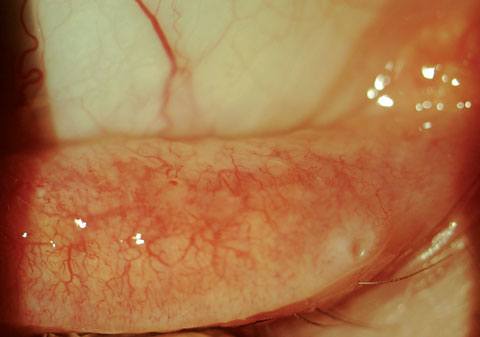
| If a patient describes the itch as being toward the eyelid, there’s a chance they’re dealing with a Demodex infection, like the patient in this photograph. |
Dry eye disease. If Demodex is ruled out, consider whether the patient has exacerbated allergies due to a poor tear film—due to either meibomian gland dysfunction or aqueous deficiency.
Is their ocular itch directed toward the caruncle, where stagnant tears—loaded with allergens and allergic mediators—have collected?5 A 2016 study in China shows an alarmingly high incidence of dry eye (98%) in young children with allergic conjunctivitis.6 More times than not, if I have a patient with both signs of dry eye disease and allergy and I lead with dry eye treatment, it reduces or, in some cases, eliminates the need for allergy treatment. With new dry eye treatments rapidly being made available, one common principle persists: if you decrease inflammation on the ocular surface and improve meibomian gland function, the tear production of most dry eye patients will improve.7 More tears means less concentration of allergens and allergic mediators on the eye, often serving as an effective treatment for the ocular allergy, which is the exact reason OTC artificial tears provide relief as well. However, they only provide temporary relief and should be used as adjunctive, not primary, treatment.
Avoid punctal plugs in patients with a history of allergy, to allow blinking to naturally flush irritants away through the punctum.
OCULAR ALLERGY DIAGNOSIS |
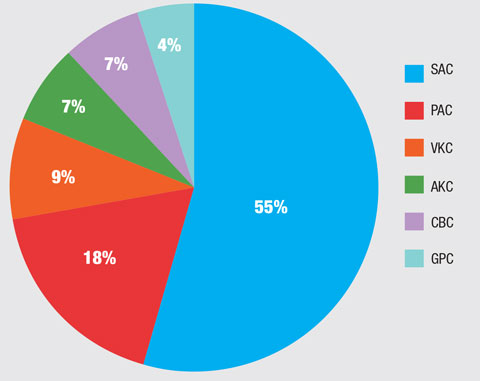 |
| Percentage of patients with a specific ocular allergy diagnosis: Seasonal allergic conjunctivitis (SAC), perennial allergic conjunctivitis (PAC), vernal keratoconjunctivitis (VKC), atopic keratoconjunctivitis (AKC), contact blepharoconjunctivitis (CBC) and giant papillary conjunctivitis (GPC).3 |
Getting a History
During the patient’s workup, investigate what symptoms related to allergies the patient has. Do they have both ocular and systemic symptoms? Patients may inadvertently take OTC allergy medications for allergy-related ocular itch, not realizing that they can actually worsen the situation. Oral antihistamines reduce aqueous and mucus production due to their anticholinergic activity, which decreases the eye’s ability to dilute allergens on the ocular surface.8 Counsel those patients about the differences and switch to a targeted ocular-allergy approach. If the patient experiences allergy-related rhinitis and other systemic symptoms, recommend OTC allergy orals, emphasizing the benefits of second-generation histamine H1 antagonists over their more ocular surface-drying first-generation counterparts.
Allergen Identification
The first rule of allergic conjunctivitis management is to identify and avoid the allergen whenever possible. While some patients know their specific triggers, the majority do not. Some clinics reported up to 80% of their allergic conjunctivitis patients had never had an allergy test before.4 In-office testing for tear osmolarity, adenovirus and MMP-9 inflammatory biomarkers have been invaluable in our viral conjunctivitis and dry eye management, as their instant results to guide our treatments. Now, there’s in-office testing to add to your ocular allergy evaluation. The Doctor’s Rx Allergy Formula (Bausch + Lomb) takes three minutes to prepare and collect patient samples without use of a needle. In less than 15 minutes, practitioners will receive the patient’s sensitivity results against 58 common allergens. In addition to these, there is also one positive and one negative control.5 If patients test negative across all allergens tested or do not show minimal response to the histamine control, they are unlikely to benefit from antihistamines or mast-cell stabilizers that inhibit histamine release.4 These patients may warrant referral to an allergist for longer-term management.
Prevalence and Characteristics of Ocular Allergy |
| In the United States, ocular allergies affect up to 40% of the population. While itching is reported in 90% of cases, the other most common symptoms—hyperemia (84.6%) and tearing (76.5%)—are also shared complaints in dry eye and other anterior segment conditions and should be differentiated. Of allergic conjunctivitis cases, 73% are largely environmental, 55% are diagnosed as seasonal allergic conjunctivitis (SAC) and 18% are perennial allergic conjunctivitis (PAC). Allergy testing for these patients is a cornerstone for treatment, as patients can be educated to develop ways to minimize their exposure and receive specific allergen immunotherapy for long-term management. The remaining 27% of ocular allergy sufferers tend to have more severe ocular reactions, from enlargened papillae to lid edema, requiring specific treatment strategies and more likely necessitate adjunctive topical steroids. 1. Leonardi A, Piliego F, Castegnaro A, et al. Allergic conjunctivitis: a cross-sectional study. Clinical and Experimental Allergy. 2015 May;45:1118-25. |
Contact Lenses
Before we discuss therapeutics, minimizing allergen exposure on the eye needs to go one step further. Fitting patients in daily disposable contact lenses is a foundation of our practice, not only due to the improved lens wear experience and convenience, but also decrease in contact lens-related complications. Of our patients fit in soft contact lenses, 90% are currently wearing a daily disposable modality. The thinking is that wearing a new lens daily will minimize allergen buildup, whereas a biweekly or monthly lens leads to buildup of allergens and irritants over time. When switching to a daily disposable is not an option due to the patient’s prescription, switching to a hydrogen peroxide cleaner in conjunction with manual cleaning (none of that “no-rub solution” business for allergy sufferers) optimizes the modality.
Allergy Therapeutics
While our arsenal of topical allergy medications has remained unchanged since extra-strength Pazeo (olopatadine 0.07%, Alcon) was released three years ago, our management of allergic conjunctivitis can continue to become more nuanced with each passing season. I recommend prescription medications in place of OTC options, as many patients seem to have already tried OTC ketotifen without relief (hence, why they are in your chair in the first place). In fact, when given both ketotifen 0.025% and olopatadine 0.1% to try on a twice-daily dose schedule, 81% preferred olopatadine, citing improved comfort and more reduction in allergy symptoms.7
The mainstays of allergic conjunctivitis therapy are topical combination antihistamine and mast-cell stabilizer eye drops. This dual mechanism provides both short- and long-term relief for its effect on decreasing histamine release. The two primary once-daily dosing topical allergy medications are Lastacaft (alcaftadine, Allergan) and Pazeo, Pataday and Patanol (olopatadine, Alcon). In a head-to-head alcaftadine 0.25% vs. olopatadine 0.2% study of 284 subjects, both topical solutions decreased itching severity within three minutes of instillation and continued to provide itch relief at 16 hours. When comparing the two, alcaftadine provided more relief.6 That said, due to olopatadine’s different available concentrations, you can customize your treatment regimen to the condition severity. Start at lower concentrations and discuss with the patient that, if more frequent dosing provides relief, the stronger formulation may be warranted.
Unfortunately, all the major ocular allergy formulations contain benzalkonium chloride (BAK) as the preservative. If you’ve ever had a patient in your chair with a laundry list of allergies, it’s not uncommon for them to be sensitive or even allergic to BAK.8 The last thing you want is for your patient to develop allergic conjunctivitis secondary to their topical allergy medication, compounding their problem. Palliative ocular allergy therapy includes allergen avoidance, cool compresses, regular linen cleaning, preservative-free artificial tears and, if warranted, short-term fluorometholone 1% ointment (non-BAK preserved).
 |
| When patients suffer from ocular inflammation due to allergy, as seen here, education about avoidance of triggers is a vital aspect of treatment. Click image to enlarge. |
Systemic Options
Depending on your state, prescribing systemic medications such as fluticasone nasal spray and oral loratadine for allergy may be additional treatment options. For patients who can’t tolerate oral antihistamines, montelukasts—while less effective—can also provide relief.9 When topical treatment alone is insufficient, consider fluticasone nasal spray or oral loratadine, but proceed with caution. While oral medications can benefit both systemic and ocular allergy, beware of increased ocular dryness due to the anticholinergic effects. If considering a steroid nasal spray, educate the patient and monitor them more often, as ocular side effects include potential increased intraocular pressure and higher risk of central serous retinopathy.10 However, if a patient’s ocular allergy is so severe that you’re considering those therapies or they’re experiencing severe systemic symptoms, comanaging with an allergist can help provide the best outcome.
Don’t Wait, Educate
Because we often only see patients once a year for their annual comprehensive eye exam (and often not during allergy season), take the opportunity during this visit to ask patients if they have a history of allergy. Begin educating patients about preventative measures and the importance of not rubbing their eyes, which further exacerbates the condition due to mast-cell degranulation and increased histamine release.11
Starting this dialogue early with patients can not only build your medical practice, but also build patient satisfaction as you preemptively take their eye care beyond the exam chair. Manage co-existing conditions, prescribe when indicated, and most importantly, identify the allergen whenever possible so patients can minimize their exposure.
Dr. Young specializes in dry eye and contact lenses at Specialty Eyecare Group in Seattle.
| 1. Kabat A, Sowka J. If it itches, it’s allergy...right? Rev Optom. 2011;147(6):107-8. 2. Mastrota K. Method to identify Demodex in the eyelash follicle without epilation. Optom Vis Sci. 2013 Jun;90:e172-4. 3. Kabat A, Sowka J. New blepharitis treatments: a decade ago, we looked at the latest treatment options for blepharitis. It’s high time we eye them up again. Rev Optom 2014;152(10):80-1. 4. Rather P, Hassan I. Human Demodex mite: The versatile mite of dermatological importance. Indian J Dermatol. 2014 Jan-Feb;59(1):60–6. 5. Lemp M, Weiler H. How do tears exit? Invest Ophthalmol. Vis Sci. 1983;24(5):619-22. 6. Chen L, Pi L, Fang J, et al. High incidence of dry eye in young children with allergic conjunctivitis in Southwest China. Acta Ophthalmologica. 2016;94:e727-30. 7. Management and Therapy Subcommittee. Management and therapy of dry eye disease: report of the management and therapy subcommittee of the international dry eye workShop (2007). The Ocular Surface. 2007;5(2):163-78. 8. Baudouin C, Labbé A, Liang H. Preservatives in eyedrops: The good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–34. 9. Gane J, Buckley R. Leukotriene receptor antagonists in allergic eye disease: A systematic review and meta-analysis J Allergy Clin Immunol Pract. 2013;1(1):65-74. 10. Haimovici R, Gragoudas E, Duker J, et al. Central serous chorioretinopathy associated with inhaled or intranasal corticosteroids. Ophthalmol. 1997 Oct;104(10):1653-60. 11. Greiner J, Peace D, Baird R. Effects of eye rubbing on theconjunctiva as a model of ocular inflammation. Am J Ophthalmol. 1985 Jul;100(1):45-50. |
