 |
Q:
I have a patient who had LASIK in the ’90s and now needs cataract surgery, but I am worried about a refractive surprise. What can I do to improve the outcome?
A:
“We now have wavefront aberrometry to improve the accuracy of IOL power selection during cataract surgery in postrefractive surgery patients,” says Lawrence Woodard, OD, of Omni Eye Services in Atlanta. In contrast to other methods, which only use preoperative corneal and axial length measurements, intraoperative aberrometry determines IOL power after the cataract is removed. “This is important because corneal topography and keratometry readings overestimate the true corneal power in post-LASIK patients. IOL calculation formulas then underestimate IOL power, leaving the patient significantly hyperopic,” says Dr. Woodard.
A 2014 study shows that 39% fewer patients’ refractions fall outside the intended postoperative target of +/- 0.50D when intraoperative abberometry was used vs. conventional preoperative methodology, notes Dr. Woodard. “This translates into happier patients who are much less likely to need an IOL exchange or enhancement procedure due to significant refractive surprise after cataract surgery.”
Measuring
It typically takes one to two minutes to obtain the measurements, so the surgical procedure isn’t significantly delayed. “Measuring is a painless process for the patient. Data from preoperative biometry is entered into the machine prior to surgery,” says Dr. Woodard.
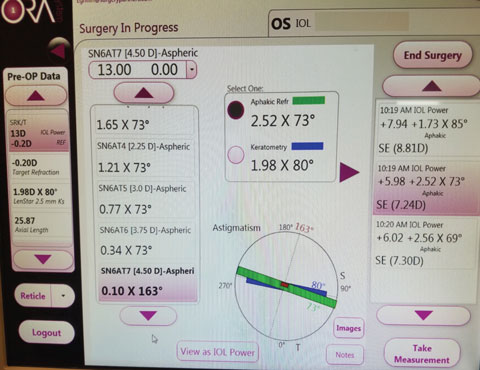 |
| ORA can be used to effectively increase the accuracy of IOL placement during surgery. |
Unfortunately, intraoperative aberrometry is not covered by insurance.
However, Dr. Woodard notes that its use is typically included in some refractive packages offered with premium lenses and laser cataract surgery. “Only a small percentage of cataract surgeons take advantage of this innovative technology, presumably due to the purchase price and monthly click fee they are charged by the company.”
Expectations center solely around increasing the accuracy of the refractive target outcome from cataract surgery, according to Robert Pinkert, OD, of Barnet Dulaney Perkins Eye Center in Phoenix. “Though the formulas used to calculate the appropriate IOL come within reach of the target, a real-time measurement that occurs during surgery can increase the predictability of the refractive result,”
says Dr. Pinkert.
Previous refractive surgeries can impact how far off you land from the refractive target post surgery, Dr. Pinkert explains. “Prior corneal surgeries, such as LASIK and RK, as well as corneal irregularities, may influence the calculations and lead to a refractive surprise—a result far from the intended target for the particular patient,” adds Dr. Pinkert.
Finally, patient expectations now focus on advancements in toric and multifocal IOL technology and intraoperative tools to help garner the most accurate refractive results. “Patients are more educated and active, thus their expectations are increasing, with a corresponding rise in the demand for better outcomes,” says Dr. Pinkert.
“My own experience did not involve prior LASIK, but I underwent surgery as a refractive lens replacement to improve my uncorrected visual acuity—I was in my fifties and way too young for cataract surgery!” says Dr. Pinkert.
“The toric lens completely neutralized the astigmatism—I am not sure this would have occurred without intraoperative verification of the IOL’s power and placement.”