 |
Q: I have several patients with inferior steepening on topography and non-specific corneal findings, suggestive of some form of non-inflammatory thinning disorder. How can I distinguish between keratoconus and pellucid marginal degeneration (PMD)?
A: PMD typically shows marked against-the-rule astigmatism on the axial map. PMD gives a characteristic topography pattern of birds kissing, a gull-winged shape or a moustache pattern, with significant invagination along the flat axis of the cornea, says optometrist Kenneth A. Lebow, of Virginia Beach, Va.
Patients who have very advanced keratoconus typically show inferior steepening. However, the topography pattern can appear similar to that of PMD, Dr. Lebow adds.
If this is the case, consider these differences: PMD corneas are typically low prolate to oblate in shape, while keratoconus corneas are almost always markedly prolate in shape. A prolate shape indicates that the center of the cornea has a steeper curvature than the periphery. The higher the shape factor, the greater the difference between the center and the periphery, as opposed to an oblate shape in which the peripheral cornea is steeper than the central cornea, Dr. Lebow says. Typically, a prolate shape factor in excess of 0.6 (numerical value) on a corneal topographer is almost diagnostic of keratoconus.
|
|
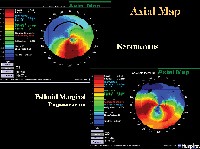
| The axial map shows a topographic similarity between keratoconus and PMD with both manifesting superior flattening and inferior steepening. Note, however, the increased invagination present with PMD. |
Two additional ways to determine which ectatic disease the patient has:
A peak elevation index (PEI).The average PEI for keratoconic eyes is about 1.95mm from the corneal apex, while the average PEI for eyes with PMD is an average of 3.5mm from the corneal apex. This is the main differentiating feature between keratoconus and PMD, Dr. Lebow says. It demonstrates that keratoconus is a mid-peripheral thinning disorder, while PMD is a peripheral thinning disorder.
To determine the peak elevation index, place the cursor over the highest elevation point on the topographers elevation map. Measure the distance from this point to the corneal apex, Dr. Lebow says.
A wavefront topographer.1 Because PMD is located inferiorly, significant trefoil is the typical finding on wavefront aberrometry. This trefoil is the optical effect of the inferior area of elevation on the topography, says Jay S. Pepose, M.D., Ph.D., of St. Louis.
In keratoconus, while the ectasia is more centrally located, its usually still inferior to the apex. So, more vertical coma is produced, reflecting this topographic asymmetry, he adds.
A small percentage of patients may actually have both conditions. In these cases, you will see a much broader area of thinning that starts almost from the center of the cor-nea or just inferior to the center, but it expands almost like a band right down to the inferior aspect of the cornea, Dr. Pepose says. Within that area, you may see two distinct zones of thinning, along with the clinical signs of both disorders.
1. Pepose J. Wavefront aberrations in patients with keratoconus and pellucid marginal degeneration. ARVO abstract #2893, 2004.
Vol. No: 142:4Issue:
4/15/05
