 A 64-year-old black male with a history of primary open-angle glaucoma presented for a follow-up examination. We diagnosed him with glaucoma four years ago. Since then, the patient has exhibited poor compliance with his follow-up schedule and topical dosing regimen. We instructed him to use 0.5% timolol BID and latanoprost QHS OU. His last eye exam was two years ago. At that time, his visual acuity was 20/20 OD and 20/30 OS. His IOP measured 9mm Hg OD and 12mm Hg OS. Additionally, his medical history was significant for medically controlled hypertension and high cholesterol.
A 64-year-old black male with a history of primary open-angle glaucoma presented for a follow-up examination. We diagnosed him with glaucoma four years ago. Since then, the patient has exhibited poor compliance with his follow-up schedule and topical dosing regimen. We instructed him to use 0.5% timolol BID and latanoprost QHS OU. His last eye exam was two years ago. At that time, his visual acuity was 20/20 OD and 20/30 OS. His IOP measured 9mm Hg OD and 12mm Hg OS. Additionally, his medical history was significant for medically controlled hypertension and high cholesterol.
At this visit, he reported that the vision in his left eye had decreased during the past six months. His best-corrected visual acuity was 20/20 OD and 20/70 OS. Confrontation fields were full to careful finger counting OD; however, he had generalized 360° constriction in the left eye. Pupils were equally round and reactive to light, with evidence of afferent defect OS. The anterior segment examination was unremarkable in both eyes. His intraocular pressure measured 19mm Hg OD and 15mm Hg OS.
Dilated fundus exam showed large cups OU, measuring approximately 0.90 OD and 0.95 OS. The vessels, macula and periphery in the right eye were normal; however, the fundus evaluation of the left eye revealed significant changes (figures 1 and 2). We also obtained an optical coherence tomography (OCT) scan and a fluorescein angiography (FA) of the left eye (figure 3).
 | |
|
1, 2. The fundus exam showed retinal hemorrhages around the left macula (OD/L, OS/R).
|
|
 |
|
|
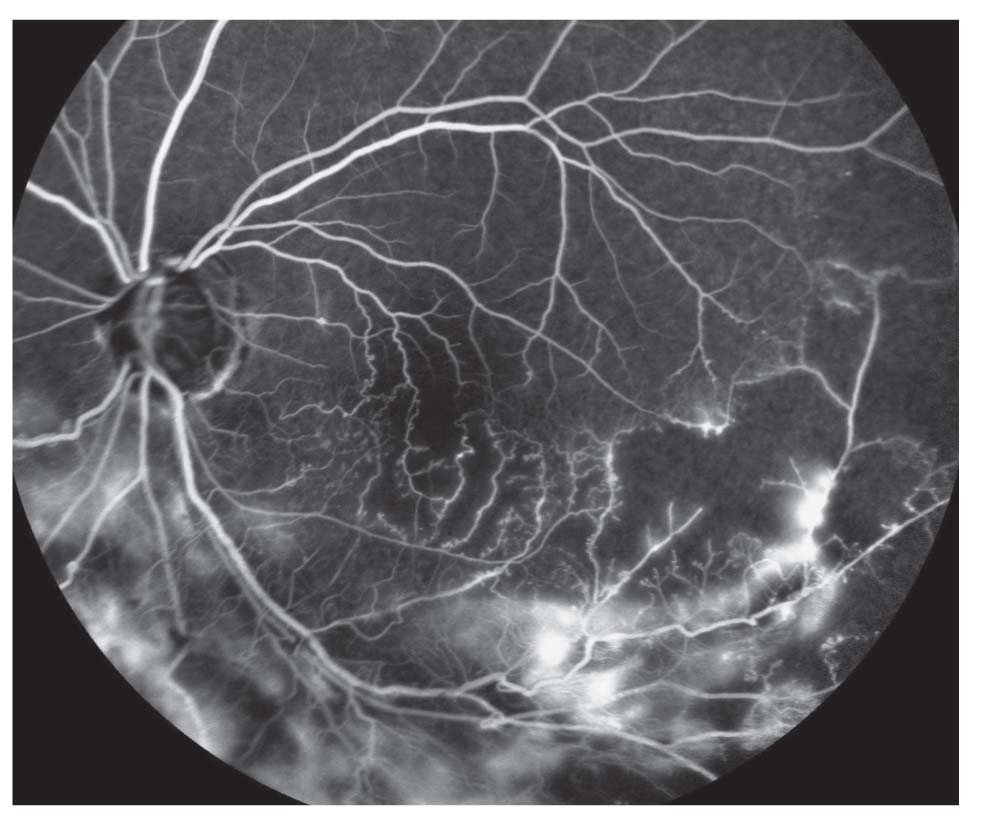
3. The late-phase fluorescein angiography showed extensive leakage in the left eye.
|
|
Take the Retina Quiz
1. What do the changes seen along the inferior arcade represent?
a. Congenital retinal telangiectasis.
b. Neovascularization with fibrous proliferation.
c. Dense epiretinal membrane.
d. Tractional retinal detachment (TRD).
2. Based on the clinical appearance, what is the correct diagnosis?
a. TRD.
b. Proliferative sickle cell retinopathy.
c. Old branch retinal vein occlusion (BRVO) with neovascularization.
d. Old branch retinal artery occlusion.
3. What is the likely cause of the reduced acuity in his left eye?
a. Macular edema.
b. Advanced glaucoma.
c. Ischemia.
d. Potentially all of the above.
4. How should this patient be managed?
a. Laser photocoagulation.
b. Intravitreal anti-VEGF
injection.
c. Observation.
d. Pars plana vitrectomy and a scleral buckling procedure.
Answers: 1) b; 2) c; 3) d; 4) a
Discussion
After looking at both optic nerves, it was evident that our patient had advanced glaucoma. Previous visual fields revealed inferior arcuate defects (OS > OD). At his last exam two years ago, the visual acuity in his left eye measured 20/30. Since then, it decreased to 20/70. Still, it was difficult to know if this was principally caused by glaucoma progression or another confounding factor.
With his history of noncompliance and advanced disease, it would be easy to assume that the visual acuity loss was a result of advanced glaucoma. But, not so fast!
A large area of fibrous proliferation that followed the inferior-temporal and inferior-nasal arcade was located inferior to the optic nerve. Within the area of fibrous tissue, we noted extensive neovascularization. In fact, the neovascularization was quite pronounced on FA testing, with a massive amount of leakage. The FA also revealed large areas of non-perfusion, which was more evident peripherally to the areas of neovascularization (especially temporally).
So, what’s the underlying cause? Based on the clinical presentation and FA, our patient had a resolved ischemic BRVO. (We noted “resolved” in the patient’s record because we can no longer see the wedge-shaped area of intraretinal hemorrhages that’s classically associated with a BRVO presentation.) While the hemorrhages weren’t evident, the retina was highly ischemic. As a result, the patient developed neovascularization.
Ischemic complications secondary to BRVO are fairly common. In 1986, the National Eye Institute’s Branch Vein Occlusion Study indicated that approximately 50% of patients with large BRVOs had significant areas of capillary nonperfusion (greater than five disc areas).1 Forty percent of those patients exhibited neovascularization, and 60% developed vitreous hemorrhages.1 The study concluded that, in patients who developed neovascularization, panretinal photocoagulation (PRP) was shown to be beneficial in preventing the development of vitreous hemorrhage.
In the era of anti-VEGF therapy, however, is PRP still the treatment of choice for neovascularization associated with ischemic BRVO? It is not clear from the literature.
The primary advantage of anti-VEGF treatment is that it swiftly resolves neovascularization. The downside is that the therapeutic effect usually is not sustained, so patients typically require multiple injections.
Further, there is a risk of tractional retinal detachments in patients with neovascularization and fibrous proliferation due to rapid involution combined with accelerated fibrosis and posterior hyaloidal contraction as a response to decreased VEGF levels.2 As a result, many retinal specialists prefer PRP or a combination of PRP and anti-VEGF therapy.
Given our patient’s history of poor compliance, we referred him for two sessions of PRP––which helped resolve the neovascularization. Other questions still remain, however, including the cause of his vision loss and why the BRVO developed in the first place.
Increased intraocular pressure is a known risk factor for the development of BRVO (and central retinal vein occlusion); however, it’s usually not considered a significant contributor until IOP reaches 30mm Hg or higher. Based on a review of his records, his IOP never increased beyond 23mm Hg.
Hypertension is the other significant risk factor in his age group. And indeed, our patient has a long history of high blood pressure––although he reported good control.
It is difficult to pinpoint the fundamental cause of our patient’s vision loss. The OCT scan revealed no macular edema, in addition to a well-preserved inner segment/outer segment junction. The FA did, however, show some ischemia––a potential contributing cause.
We have not performed a visual field test since the development of the BRVO. Presently, our chief goal is to reduce the patient’s IOP as much as possible. We repeatedly stressed the importance of medication compliance, and scheduled him for a one-month follow-up appointment. Fortunately, the patient heeded our advice––his IOP measured 10mm Hg OU at the follow-up. Now, we simply have to wait until we can perform another visual field test after the BRVO stabilizes completely.
1. Branch vein occlusion study group: Argon laser photocoagulation for prevention of neovascularization and vitreous hemorrhage in branch vein occlusion. Arch Ophthalmol. 1986 Jan;104(1):34-41.
2. Arevalo JF, Maia M, Flynn HW Jr, et al. Tractional retinal detachment following intravitreal bevacizumab (Avastin) in patients with severe proliferative diabetic retinopathy. Br J Ophthalmol. 2008 Feb;92(2):213-6.
