 |  |
Innovations in presbyopia correction are popular in eye care today, and for good reason: the population of those over 65 is expected to almost double from 43.1 million in 2012 to 83.7 million in 2050.1
Intraocular lens (IOL) manufacturers have been pursuing this market for over 30 years, with varying degrees of success. No lens can give everyone complete freedom from glasses both at distance and near, but careful patient selection combined with surgical expertise can bring more people than ever closer to that goal for most visual tasks. Newer designs that have increased our success include improved aspheric lenses, methods to increase depth of focus and diffractive concentric rings in a trifocal design. The Tecnis Synergy IOL by Johnson & Johnson Vision is the latest entrant. Available internationally since 2019, it was recently FDA-approved for use in the US.
Synergy combines elements of two earlier J&J lenses—the Tecnis Multifocal (a trifocal) and the Tecnis Symfony (an extended depth of focus, or EDOF, lens). In this way, the Synergy aims at giving patients the widest range of continuous vision, as well as minimizing nighttime photopic phenomena that have been historically reported with most multifocal IOLs.
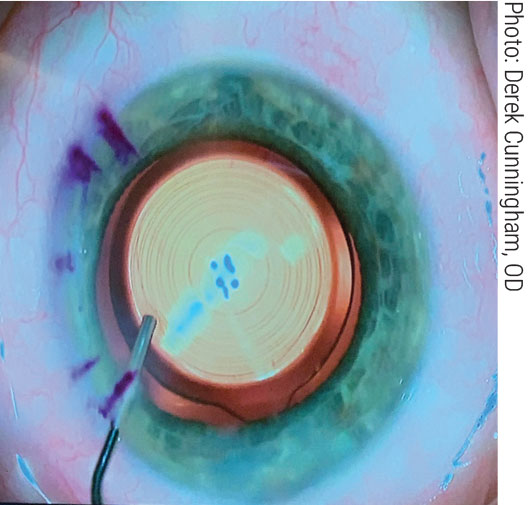 |
The Synergy aims to give patients a wider range of vision by combining two optical concepts. Click image to enlarge. |
In a J&J-funded case series involving 103 patients undergoing bilateral implantation of the Synergy lens, 96% of subjects achieved 20/20 uncorrected binocular distance acuity and 91% uncorrected near acuity.2 Mean monocular and binocular uncorrected near acuity was 0.09±0.03 logMAR and 0.04±0.02 logMAR, respectively. Mean mesopic uncorrected near acuity was a bit worse compared with photopic light conditions at 0.14 ±0.03 logMAR, as is typical with trifocal lens designs. Still, it is worth noting these differences tended to be smaller than with other trifocals.
By reducing reliance on diffractive optics, the Synergy may become a viable option for more patients. Historically, trifocal lens designs have required the most pristine eyes with virtually no ocular disease affecting the integrity of the visual pathway due to their diffractive nature. Non-diffractive EDOF lenses are more forgiving of comorbidities such as epiretinal membranes, Fuchs’ dystrophy, irregular astigmatism and macular degeneration. Synergy does include diffractive optics but in a smaller range of focal lengths, relying instead on EDOF for improved near to intermediate vision; proponents say this approach has the potential to reduce incidence of halos around lights at night.
Another thing to consider due to these EDOF properties is the ease of which it is to over-minus patients when refracting. Be aware of this and try to push as much plus power as possible.
Top Two Factors
It is still of utmost importance to consider lifestyle factors when recommending Synergy or any other presbyopia-correcting IOL for patients. As the physician, ask questions regarding occupation and hobbies to properly assess a patient’s visual demands. You should also gauge their personality when conversing with them in your chair. It has been shown that the personality of the patient is one of the leading factors in determining success with a multifocal IOL, with two of the most important traits being conscientiousness and agreeableness.3
Secondly, surgical skill is equally critical to patient satisfaction, as any residual refractive error or induced astigmatism will manifest in the patient’s visual experience. As always, choose your surgeon wisely.
Dr. Zimmerman is an ocular disease resident at Dell Laser Consultants in Austin, TX. He has no financial disclosures.
Dr. Cunningham is the director of optometry at Dell Laser Consultants in Austin, TX. He has no financial interests to disclose. Dr. Whitley is the director of professional relations and residency program supervisor at Virginia Eye Consultants in Norfolk, VA. He is a consultant for Alcon.
1. Ansari Z, Miller D, Galor A. Current thoughts in fungal keratitis: diagnosis and treatment. Curr Fungal Infect Rep. 2013;7(3):209-18.
2. Pepose JS, Wilhelmus KR. Divergent approaches to the management of corneal ulcers. Am J Ophthalmol. 1992;114:630-2.
3. Jones DB, Sexton R, Rebell G. Mycotic keratitis in South Florida: a review of thirty-nine cases. Trans Ophthalmol Soc U K. 1970;89:781-97.
