 |
A 65-year-old Hispanic female presented with a chief complaint of blurred vision at distance and near that had persisted for one year. Her medical history was significant for controlled hypertension and type 2 diabetes.
On examination, her best-corrected visual acuity measured 20/20-2 OD and 20/20- OS. Ocular motility testing was normal. Confrontation visual fields were full to careful finger counting OU. Her pupils were equally round and reactive, with no evidence of afferent defect OU. The anterior segment examination was significant for 2+ nuclear sclerotic cataracts in both eyes.
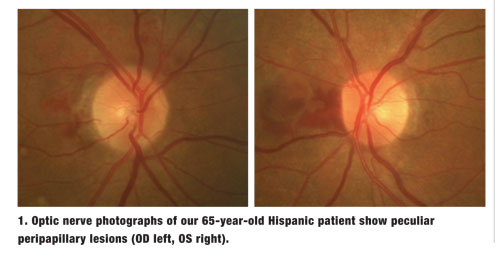
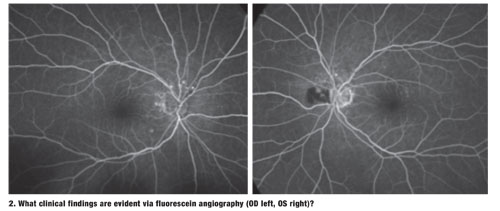
Dilated fundus exam revealed flat and clear maculae, with a positive foveal reflex OU. Upon examination of the nerves, we noted minimal cupping with good rim coloration and perfusion. However, we documented peculiar lesions located adjacent to both optic nerves (figures 1 and 2). We also performed a fluorescein angiogram (figures 3 and 4).
Take the Retina Quiz
1. Based on the optic nerve head photographs and fluorescein angiogram, the peripapillary lesions are most consistent with:
a. Hemorrhagic pigment epithelial detachments.
b. Intraretinal hemorrhages and exudation.
c. Choroidal neovascular membranes.
d. Intraretinal edema and subretinal hemorrhages.
2. What is the correct diagnosis for this condition?
a. Coats’ disease.
b. Cystoid macular edema.
c. Diabetic papillopathy.
d. Polypoidal choroidal vasculopathy (PCV).
3. Which ancillary test is the standard of care for confirming the presence of this condition?
a. Fluorescein angiography (FA).
b. Indocyanine green (ICG) angiography.
c. Optical coherence tomography.
d. B-scan ultrasonography.
4. How should this patient be managed?
a. Laser photocoagulation.
b. Photodynamic therapy.
c. Intravitreal anti-VEGF injection.
d. Observation.
Discussion
We diagnosed our patient with polypoidal choroidal vasculopathy. This condition was first described by Lawrence A. Yannuzzi, MD, and associates in 1982, and was shown to cause multiple, recurrent, serosanguineous detachments of the retinal pigment epithelium (RPE) and the neurosensory retina.1
Since initial discovery, the disease has been given several different names, including “idiopathic polypoidal choroidal vasculopathy,” “posterior uveal bleeding syndrome” and “multiple serosanguineous retinal pigment epithelial detachment syndrome.” Today, the condition is universally known as PCV, and is recognized as a unique form of occult choroidal neovascular membrane.2
PCV is characterized by branching choroidal networks that terminate in outward-reaching vessel projections. Clinically, these vascular networks appear as reddish-orange, polyp-like structures. The nodular lesions are associated with serous exudation and hemorrhage, as well as pigment epithelial and neurosensory detachments. Additionally, vitreous and subretinal hemorrhages are common features.
The condition principally manifests in the macular and peripapillary areas.3 When it occurs in the macula, some clinicians misdiagnose PCV as AMD.
However, in stark contrast to macular degeneration, PCV tends to occur in darker pigmented individuals. In fact––although researchers haven’t yet determined the true incidence of PCV in blacks––some studies suggest that nearly all African-American patients who present with “neovascular AMD” likely have PCV.2
Initially, researchers believed that PCV occurred exclusively in black females. But, we now know that the condition affects both males and females of several pigmented races, including Hispanics and Asians. For example, one study indicated that 54.7% of Japanese patients previously diagnosed with neovascular AMD actually had PCV.4
Fluorescein angiography, ICG angiography and spectral-domain optical coherence tomography are the most useful ancillary tests for diagnosing PCV. It is worth noting that ICG angiography can be more effective for visualizing PCV than FA. This is because indocyanine green absorbs and emits near-infrared light, which penetrates the RPE and allows the practitioner to see choroidal abnormalities, branching networks of inner choroidal vessels and focal nodular areas of hyperfluorescence arising from the choroidal circulation.3 Fortunately, we were able to appreciate these changes in our patient using fluorescein angiography alone.
Appropriate management of PCV is dictated by several disease variables, including location (peripapillary vs. macular), lesion size, and the presence of secondary bleeding and/or exudation. However, for those who develop vision loss as a result of sersosanguineous RPE and neurosensory retina detachments, laser photocoagulation can be used. (Laser treatment is only recommended when the entire polypoidal lesion can be treated effectively.2) Because thermal laser causes retinal damage, directly targeting the choroidal vessels via photodynamic therapy (PDT) is preferable.
Intravitreal anti-VEGF injection for PCV may help resolve macular edema, as well as provide a modest decrease in polypoidal complexes. However, recent studies evaluating a combination of PDT and anti-VEGF therapy have documented more pronounced polyp regression when compared to anti-VEGF injection alone.3
Because our patient presented with non-visually significant peripapillary lesions, her retinal specialist opted for observation at this time. We will schedule her for a follow-up evaluation in our office in four to six weeks.
Thanks to Angela DiMarco, OD, optometric resident at Bascom Palmer Eye Institute in Miami, for contributing to this case.
1. Yannuzzi LA, Sorenson J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy. Retina. 1990;10(1):1-8.
2. Imamura Y, Engelbert M, Iida T, et al. Polypoidal choroidal vasculopathy: A review. Surv Ophthalmol. 2010 Nov-Dec;55(6):501-15.
3. Ryan SJ, Sadda SR, Hinton DR. Polypoidal Choroidal Vasculopathy. Retina, 5th Ed. London: Elsevier, 2013;1285-90.
4. Maruko I, Iida T, Saito M, et al. Clinical characteristics of exudative age-related macular degeneration in Japanese patients. Am J Ophthalmol. 2007 Jan;144(1):15-22.
