 |
| Our 10-year-old patient presented with blurred vision in both eyes and a large-angle exotropia in the left eye. What is the likely diagnosis?
|
Her best-corrected visual acuity measured 20/60 OD and 20/200 OS. Upon near testing, she improved to 20/30 OD, but exhibited no clinically significant acuity gain in her left eye.
Confrontation fields were full to careful finger counting OU. Her pupils were equally round and reactive, with no evidence of afferent defect OU.
She had an obvious, large-angle exotropia in her left eye that measured more than 40 prism diopters. The anterior segment evaluation was unremarkable OU.
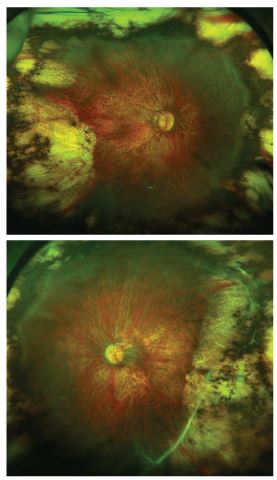
The dilated fundus exam revealed obvious changes (see page 86). We noted extensive chorioretinal scaring in the peripheral retina, without evidence of detachment in either eye.
Take the Retina Quiz
1. Based on the history and clinical findings, our patient most likely:
a. Has a history of blunt force trauma.
b. Was born premature.
c. Has a younger brother with poor vision.
d. Has congenital tumors in both eyes.
2. How do you explain the peripheral fundus findings?
a. Regressed retinoblastoma.
b. Evidence of severe myopic degeneration.
c. Old rhegmatogenous retinal detachment.
d. Laser scars.
3. Which factor likely is principally responsible for the patient’s underlying ocular condition?
a. High myopia.
b. Genetic predisposition.
c. Low birth weight.
d. Supplemental oxygen use.
4. What is the nature of our patient’s exotropia?
a. Congenital.
b. Sensory.
c. Weak medial rectus muscles.
d. Weak lateral rectus muscles.
5. What is the most effective way to manage this patient?
a. Contact lens fitting.
b. Vitrectomy and a scleral buckling procedure.
c. Observation.
d. None of the above.
Discussion
Our patient was born at gestational week 24, and weighed just 1lb, 6oz. She received oxygen therapy for three months, and was subsequently discharged at five months of age, weighing 7lbs, 9oz.
The patient was screened for retinopathy of prematurity (ROP) at both seven and nine weeks of age, and exhibited no signs of retinal damage. However, by week 10, stage 2 ROP was noted in both eyes. Just one week later, the ROP progressed to threshold stage 3 with evidence of “plus disease.” In an effort to halt disease progression, she received three sessions of laser photocoagulation.
We determined that our patient experienced ROP regression, as well as the secondary effects of extensive laser treatment to the peripheral retinas.
Retinopathy of prematurity is a vasoproliferative disease that characteristically occurs in premature infants. It is the leading cause of blindness in infants less than one year of age.1 The key pathologic feature is retinal ischemia, which can precipitate significant neovascularization.
Our understanding of ROP’s pathophysiology has improved dramatically in the last 75 years. When initially discovered in 1942, ROP was termed “retrolental fibroplasia.” At that time, clinicians only could confirm that the condition was the primary cause of childhood blindness.
By the 1950s, researchers documented a relationship between supplemental oxygen use and ROP development. Therefore, many hospitals gradually ceased prescribing oxygen therapy to premature neonates. Unfortunately, many premature infants who did not receive supplemental oxygen subsequently developed respiratory distress syndrome (RDS).1 It wasn’t until the late 1960s and early 1970s that arterial blood gas analysis was developed, which markedly reduced the incidence of RDS.
While supplemental oxygen certainly is linked to a higher incidence of ROP, we now know that low birth weight is the primary risk factor.1 Specifically, 75% of ROP cases are diagnosed in neonates who weigh less than 2.2lbs (1,000g) at birth.1 In fact, it is exceedingly rare to document ROP in newborns who weigh more than 2.75lbs (1,250g).1
The classification of ROP is based on disease location, extent and severity:
• Stage 1 features a ridge in the periphery.
• Stage 2 shows evidence of a demarcation line.
• Stage 3 is a demarcation line associated with fibrovascular proliferation.
• Stage 4 features a partial retinal detachment.
• Stage 5 constitutes a total retinal detachment.
Plus disease signifies a more florid form of ROP, and typically presents with retinal vessel dilation and tortuosity, iris vascular engorgement, pupillary rigidity and vitreous haze. ROP patients who exhibit plus disease usually receive a worse visual prognosis.
It is important to note that 90% of ROP cases will spontaneously self-resolve without treatment. Further, just 10% of ROP will progress beyond stage 3. Although cryotherapy has been shown to effectively treat advanced stage 3 disease, binocular laser indirect ophthalmoscopy photocoagulation is now used more frequently because of its lower propensity to induce postoperative sequelae (e.g., inflammation and swelling).1 Retinal detachment surgery is indicated for stage 4 macula-off retinal detachment and stage 5 ROP.
Because the contemporary survival rate of low birth weight infants is so high, eye care providers likely will continue to see more ROP cases than ever before. Affected individuals often present later in life with unusual retinal findings. Although our patient’s clinical findings are fairly extreme, most ROP patients will exhibit some evidence of macular dragging, vitreoretinal fibrosis, lattice degeneration, and even retinal holes or tears. Keep in mind that advanced ROP patients are at an elevated lifetime risk for retinal detachment.
The retinal changes observed in our patient were stable. We referred her to a contact lens specialist for a fitting, which was successful. She and her mother returned to our office for a follow-up, and reported significantly improved vision and increased performance in school. Upon contact lens correction and an over-refraction, her vision was 20/50 at distance and J2 at near OD. Unfortunately, her acuity remained 20/200 OS.
Her mother remained concerned about the exotropia––which we believed was of a sensory nature. So, we referred the patient for a strabismus surgery consultation.
Answers: 1) b; 2) d; 3) c; 4) b; 5) a.
1. Lee TC, Chiang MF. Pediatric Retinal Vascular Diseases. In: Ryan SJ, Schachat AP, Murphy RP (eds.). Retina, Vol. II: Section 2, Chapter 61. Retinal Vascular Disease. 5th ed. St. Louis: Mosby; 2013:1108-28.
