 Q: I see a lot of patients with dry eye who, upon questioning, also say they have dry mouth. What’s my next step in ruling out Sjögren’s syndrome?
Q: I see a lot of patients with dry eye who, upon questioning, also say they have dry mouth. What’s my next step in ruling out Sjögren’s syndrome?
A: “It’s all about history,” says Robert Prouty, OD, center director of Omni Eye Specialists in Denver. “There’s no one specific sign or symptom that is uniquely diagnostic for Sjögren’s syndrome.”
That said, the hallmark symptoms of Sjögren’s are dry eye and dry mouth (xerostomia). Indeed, a recent study found that almost 12% of patients with aqueous-deficient dry eye have Sjögren’s syndrome.1
So, Dr. Prouty says, if you see a patient with dry eye who also reports dry mouth, or is holding onto a water bottle, ask about:
- Joint pain/dysfunction.
- Dental problems.
- Gastrointestinal issues.
- Neurological symptoms (“brain fog”).
 |
| Superficial punctate keratitis in a Sjögren’s patient on Restasis therapy. |
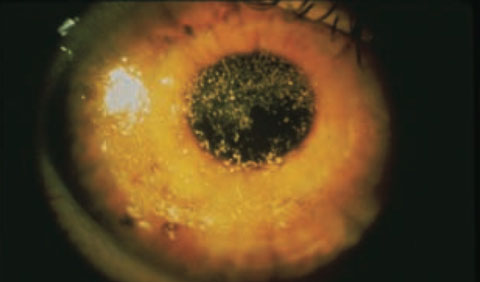 |
| Severe filamentary keratitis in a mucus sheet in a patient with severe dry eye due to Sjögren’s. |
Any of these conditions should prompt you to investigate further. Unfortunately, because the symptoms of Sjögren’s are non-specific, it can take more than six years after the onset of symptoms before the patient is diagnosed, according to the Sjögren’s Syndrome Foundation. Thus, the optometrist is in a key position to get these patients diagnosed early, and to help them obtain treatment.
Now, who do you refer them to?
“I don’t think that sending the patient to the primary care physician or family doctor is always the best choice,” Dr. Prouty says. The family doctor may not have the familiarity with the disease to put the patient on a quick course to diagnosis.
A better option is to send the patient to a rheumatologist or dentist who has experience or knowledge in diagnosing Sjögren’s or other autoimmune diseases.
The time to find an experienced rheumatologist or dentist is now, before you have a patient with Sjögren’s in your chair, Dr. Prouty says. “Ask around to find a qualified doctor you can work with—one who has the diagnostic know-how to do advanced workup and histologic testing,” he says.
Diagnostic blood work usually involves anti-nuclear antibody (ANA), autoantibodies (Anti-SSA or Anti-SSB) and rheumatoid factor tests. Additional dental testing may include measuring salivary gland function or salivary gland/lip biopsy (“lip punch”) for lymphocytic infiltration.
While the patient may have no joint symptoms, referring to a rheumatologist is still the right call, Dr. Prouty says. That’s because a rheumatologist is the one who is most likely to be familiar with the systemic medications to treat the patient. For Sjögren’s, that means immunosuppressive medications such as methotrexate or Plaquenil (hydroxychloroquine, Sanofi-Aventis).
Meanwhile, the optometrist should be treating and monitoring the patient’s ocular health. Dry eye is usually chronic in patients with Sjögren’s, and can even be sight threatening if it becomes very severe, Dr. Prouty says. Treatment involves frequent administration of artificial tears (preferably non-preserved), and possibly Restasis (cyclosporine, Allergan) for long-term control of inflammation.
Last but not least, “the optometrist should be working in concert and inter-reporting with the rheumatologist, and the dentist as well, to confer about keeping the patient’s condition stable,” Dr. Prouty says.
1. Liew MS, Zhang M, Kim E, Akpek EK. Prevalence and predictors of Sjogren’s syndrome in a prospective cohort of patients with aqueous-deficient dry eye. Br J Ophthalmol. 2012 Dec;96(12):1498-503.
