As far as dry eye disease (DED) treatment goes, the times are a-changing. Not long ago, an optometrist would have said a patient with no symptoms of DED had no DED. But as research continues to show that DED signs and symptoms don’t necessarily correlate, clinicians must turn to other markers for a diagnosis.1,2
Here, we examine several of the underlying conditions that could be causing patients’ itchy, stinging, dry eyes.
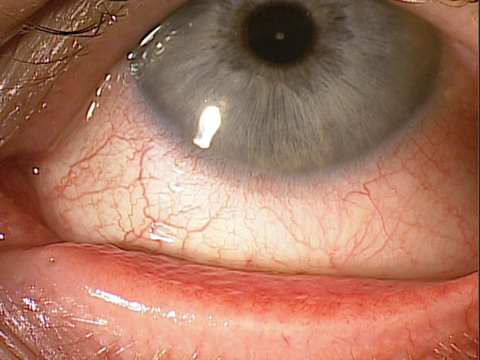 |
| This patient’s red, irritated eye is a classic sign of allergic conjunctivitis. Click image to enlarge. |
Case Example
A patient presents reporting symptoms of dryness, such as grittiness and irritated red eyes, that typically occur late in the day or after computer use. That seems like a pretty straightforward diagnosis for DED, especially since meibomian gland expression shows mild turbid secretions. The patient also displays mild inferior corneal staining. He was previously placed on topical anti-inflammatory medications and a lipid-based tear. After three months, omega fatty acids were added and, at six months, punctal plugs. In frustration, the patient discontinued all medications and scheduled an appointment. Upon examination, the patient mentioned the exact same symptoms: dry, gritty, red and irritated eyes late in the day and especially while on the computer. At this examination, he was tested for osmolarity with the TearLab Osmometer (TearLab) and measured 293 OD and 291 OS. The expression was similar, as was inferior corneal staining. There was no lissamine green dye staining of the conjunctiva, and the tear meniscus height was normal. Noninvasive tear break-up time (TBUT) took longer than 10 seconds.
We relied on the combination of these more advanced tests and point-of-care diagnostics and were quickly able to see that this was not DED at all. Cover testing revealed exophoria at distance and convergence insufficiency at near. The patient also had a positive tight lid seal test in both eyes, indicating that his eyelids do not completely seal, especially at night.
He was told to discontinue using a ceiling fan at night and to use lid hygiene products and a hydrating compress for mild blepharitis. He was given the option of vision therapy and prescribed a new pair of progressive lenses with base in prism for his exophoria/convergence insufficiency. Within a week, the patient’s symptoms were gone and he was able to work on the computer with comfort; he even commented that, not only did his dry eye symptoms disappear, but he rarely experiences headaches anymore.
This case shows the importance of using advanced, sensitive testing and realizing there are many other conditions that have symptoms similar to dry eye that are not dry eye.
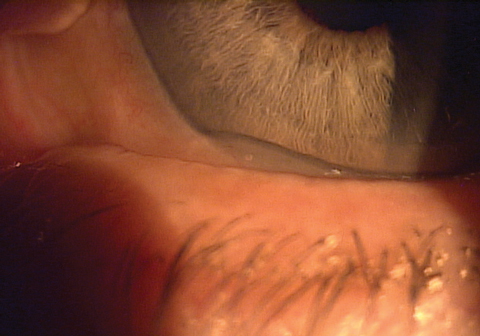 |
| Conjunctivochalasis, seen here, can look like or, in some cases, lead to, dry eye. |
Conjunctivochalasis
This condition can eventually lead to DED, but in most stages it is unrelated and typically causes symptoms of grittiness, foreign body sensation, epiphora and red, irritated eyes. Conjunctivochalasis (CCH) usually tests positive for corneal and conjunctival staining and a rapid TBUT, but in mild-to-moderate cases, osmolarity is normal while MMP-9 testing can be elevated.3-5
The presence of more frequent subconjunctival hemorrhages may point to CCH, but the overlap with DED represents yet another reason to initiate advanced OSD testing.6 The symptoms are quite similar to dry eye; however, in CCH the hallmark symptom is pain or foreign body sensation in a localized area. Patients have the ability to pinpoint it, like when they have an eyelash in their eye. Most commonly, they feel it when they blink or with eye movement.7 In fact, a clinician can reproduce pain with local pressure by pressing on the lids over the area of conjunctival chalasis while the patient looks in the opposite direction. This condition is sometimes confused with DED. Further complicating matters, many CCH patients experience epiphora secondary to the redundant conjunctival tissue, which prevents tear flow to the punctum. Also, DED can worsen in the presence of CCH, making the distinction more difficult.8 This is important because in advanced cases of CCH there is likely a comorbidity of DED. Advanced cases of CCH also can result in exposure problems.8 Another characteristic of conjunctivochalasis is that almost all cases occur in the temporal and sometimes central conjunctiva.7
The actual condition is characterized by loose or redundant conjunctival tissue and may be associated with absence or stretching of subconjunctival tenons fascia. Histology slides of CCH show the presence of lymphangiectasia. The chronic prolonged mechanical obstruction of lymphatic flow may result in lymphatic dilation and eventually give rise to CCH. Inflammation plays an important role in the pathogenesis of CCH, and pooling of inflammatory cytokines in tears of patients with chalasis has been shown to induce distinct adverse effects that compromise the patient’s ocular surface health.5
Risk factors for CCH include age (older than 50), a history of DED, prior ocular surgery or a history of conjunctival chemosis. Conditions that may cause conjunctival chemosis include long-standing allergic conjunctivitis, dry eye, trauma or inflammatory conditions such as episcleritis.9
Research also suggests an association between conjunctivochalasis and immune thyroid disease.10 A prospective study found that the prevalence of CCH in patients with autoimmune thyroid eye diseases was as high as 88%.10 It is imperative for optometrists to rule out an association with thyroid disease and to have systemic management be initiated by an endocrinologist.
 |
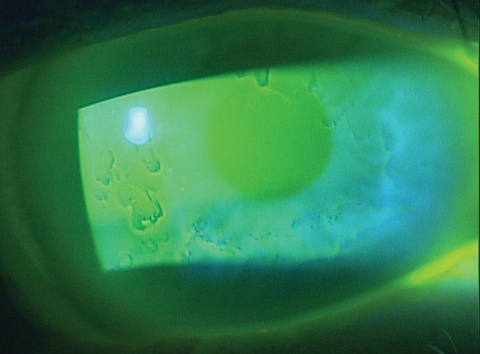 |
| Gritty, dry eyes is a symptom of epithelial basement membrane dystrophy, a common anterior segment issue. |
Salzmann’s Nodular Degeneration
Research shows this can mimic dry eye.11 Salzmann’s nodular degeneration (SND) histopathology reveals that the epithelium over the nodules is considerably thinned, resulting in symptoms of dryness, foreign body sensation, gritty eyes and irritation.11 The most common symptom is blurred vision.2 SND is bilateral in 63% of cases.12 Studies show that approximately 40% of patients with SND also have meibomian gland disease (MGD).12,13 SND has also been linked to inflammation and even inflammatory systemic conditions, such as Crohn’s disease.13 Treatment typically involves surgical removal, as these tend to exist in the peripheral cornea.
Blepharitis
Infections, including staphylococcal and Demodex, can cause itching, irritation, dryness and blurred vision.14
Eventually, this inflammation will lead to MGD, resulting in potential DED; thus, mechanical treatment will often stave off the progression caused by the biofilm.15 But blepharitis can also exist on its own, without inducing dry eye disease in many cases—especially early cases. One poster presented at the TFOS conference in Montpellier, France in September 2016 shows the three most common conditions in patients with symptoms of DED but normal osmolarity are allergic conjunctivitis, blepharitis and epithelial basement membrane dystrophy (EBMD). Patients with blepharitis—especially as a result of Demodex—will complain of itchy, gritty eyes, although the itching is typically localized to the lid margin/lash area.16
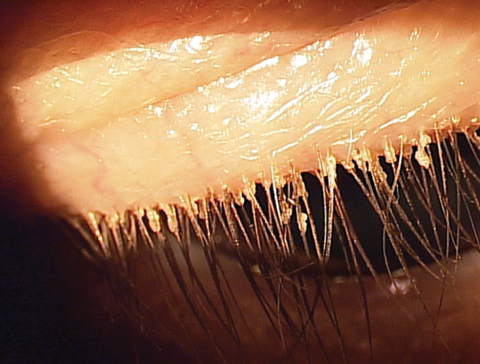 |
| A close examination of the lashes reveals the cause of this patient’s blepharitis—Demodex. |
Epithelial Basement Membrane Dystrophy
This is one of the most common anterior segment conditions an eye care physician will observe in clinical practice.17 Although many patients with EBMD may be asymptomatic, patient symptoms range from blurred visual acuity (VA) and gritty, dry eyes to severe pain and recurrent corneal erosion (RCE). EBMD affects nearly 42% of individuals across all age groups, and up to 33% of patients with EBMD experience RCE during their lifetime.18,19
The clinical signs of EBMD typically include a bilateral presentation of epithelial microcysts and whirling superficial defects, such as corneal ridges and opacities. EBMD is not considered an inherited condition, but several reports show otherwise.20,21 In one study, researchers identified two different point mutations in the genes associated with other corneal dystrophies.20 EBMD is associated with a faulty basement membrane, which is thickened, multilaminar or redundant, and misdirected into the epithelium. The basal epithelial cells manufacture either unconventional redundancies or finger-like projections that protrude from an abnormally thickened basement membrane.21
Dryness is one of the more common symptoms of EBMD, and patients may report fluctuating vision, grittiness or photophobia.22 A slit lamp examination can reveal the presence of microcysts, which are epithelial cells trapped in intercellular debris in the redundant basement membrane formation. These microcysts can be observed best with fluorescein staining and often appear as inverse or negative staining areas. A slit lamp examination may reveal the classic identifying maps, dots, lines and even fingerprint-type formations.
 |
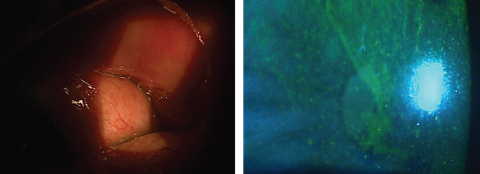
| This patient’s irritation may have felt similar to dry eye, but MMP-9 testing shows an underlying giant papillary conjunctivitis. |
A Question of Comfort
Contact lens discomfort typically results in symptoms of dry eye disease, but dissipates when the contact lens is not worn. The cause could range from subclinical DED and MGD to issues with the contact lens itself, solutions or compliance. Daily disposable lenses and higher quality materials that retain moisture are often the best options for these patients, as well as contact lens solutions containing hyaluronic acid or other lubricating agents.
Patients should be observed for partial blinking habits and MGD and should be tested with more sensitive testing, such as noninvasive TBUT, osmolarity and lissamine green dye staining.
Giant Papillary Conjunctivitis
Other contact lens complications, such as giant papillary conjunctivitis (GPC), can result in symptoms that can range from decreased contact lens wearing time to foreign body sensation to irritated, dry eyes with ropy, clear discharge.23 Making the differential even more difficult, one study shows that patients with GPC have greater levels of meibomian gland dropout in both lower eyelids and that the meibum expressed from patients with GPC is more viscous than patients without GPC.24
Testing for GPC typically shows normal osmolarity, but increased MMP-9 levels.25 These patients often have a history of contact lens wear, but lack compliance, usually wearing lenses beyond the two weeks or one month time frame indicated. Everting their eyelids will show large papillae and hyperemia without corneal or bulbar conjunctival involvement.
Conjunctivitis
Even conjunctivitis itself can seem like DED. Studies show that patients with DED also suffer from symptoms such as itching and dryness, especially in the case of allergic conjunctivitis patients.26 Differentiating these two conditions requires an astute clinician. Investigators have found that the more common oral pharmaceutical agents for allergy treatment have a significant drying effect on the ocular surface and can actually induce dry eye.27 That dry eye can allow allergens to remain on the surface longer and may exacerbate the allergic conjunctivitis. Compounding this is the realization that symptoms of DED may be quite similar to those of allergic conjunctivitis.
In one study, clinically significant itching was found in 28.2% of allergic conjunctivitis cases, dry eye as a symptom found in 35.8% and redness in 28.2%.26 An ideal way of making a differentiation is to look to the more classic allergic conjunctivitis clinical findings, such as conjunctival papillae, conjunctival chemosis or eyelid edema or a combination or all three.28 A key systemic differentiator is rhinitis, which is present in more than 80% of cases of allergic conjunctivitis, but is not a symptom known to be associated with dry eye disease. Other findings found in patients with allergies include as strong family history, atopic dermatitis or the presence of asthma.28
Floppy Eyelid Syndrome
Many patients with this diagnosis will also develop DED; however, DED will not resolve with standard treatment unless the loose eyelids are addressed. Floppy eyelid syndrome (FES) is characterized by chronic superficial keratitis, MGD, corneal abrasions, giant papillary conjunctivitis and mucous discharge.29 Most tellingly, when the upper eyelid is everted, affected lids are rubbery and may even flop easily or have a history of spontaneous eversion. Because FES is directly linked to sleep apnea and obesity, test for associated systemic conditions, such as diabetes and hypertension.30
Management for FES typically involves treating the components of the disease with anti-inflammatory medications, lubricants and lid hygiene and referring to an oculoplastic surgeon for eyelid repair or tightening.
Limbal Stem Cell Deficiency
These patients will often complain of blurred or fluctuating vision associated with photophobia and dry, irritated eyes.31 The typical causes include chemical burns and severe ocular scarring secondary to conditions such as Stevens-Johnson syndrome.32
A diagnosis of limbal stem cell deficiency (LSCD) is made if corneal epithelium damage results in a dysfunctional stem cell population. The final outcome is an inability to produce healthy epithelium. The key signs of LSCD are corneal haze, conjunctivalization, epithelial irregularity and superficial neovascularization of the cornea.33 Typically, these signs begin with the superior cornea and then move centrally.34 In addition to chemical burns and Stevens-Johnson, other causes of LSCD include contact lens-induced keratitis, aniridia, multiple ocular surgeries, peripheral ulcerative disorders, chronic neurotrophic keratitis, pterygium, severe microbial keratitis, chronic bullous keratopathy and radiation therapy.33 In cases with no pathology or history of trauma, question the patient about contact lens abuse.35
In addition to evaluating the clinical picture, a conclusive diagnosis of LSCD can be made via impression cytology. Although not a readily available test, the hallmark finding of conjunctivalization reflects the presence of goblet cells in that area of the cornea and cytokeratine-19 positive cells.36 Furthermore, a statistically significant percentage of patients with LSCD also have decreased corneal sensitivity.37
 |
| At left, this patient’s dry eye symptoms won’t resolve until the underlying floppy eyelid syndrome is treated. At right, this patient’s LSCD could be due to chemical burns and severe ocular scarring secondary to conditions such as Stevens-Johnson syndrome. Click image to enlarge. |
Mimickers Roundup
Besides the ocular conditions mentioned above, many others can mimic DED symptoms. These include conjunctival concretions that result in foreign body sensation and irritation. Removal of exposed concretions typically relieves the patient’s symptoms. Less common causes include superior limbic keratoconjunctivitis, an allergy to a chronic medication such as brimonidine in glaucoma treatment or even reactions to preservatives in other chronic topical medications. Patients with raised pterygia or pinguecula can have dry, irritated, red eyes with burning and fluctuating vision; keep in mind that arid conditions and UV exposure can cause the formation of pinguecula and pterygia. Even exposure keratopathy in patients with lagophthalmos or previous eyelid cosmetic surgery procedures can develop inferior corneal staining, even though their tear film may not be affected at first. Eventually, it leads to MGD and DED.
As clinicians, it’s imperative that we look at more technologies and use multiple tests in the diagnosis of DED. Relying on symptoms alone will likely frustrate both the patient and doctor. The advantage of multiple tests—especially more sensitive ones such as osmolarity, non-invasive tear break-up time measurements, meibography and even lissamine dye staining—is that they can help specify the precise type of DED, when performed in concert with slit lamp examinations and a comprehensive patient history. At the same time, running too many tests or performing too many procedures or treatments can make things difficult on patients and costly. Selecting the right tests to arrive at a confirmatory diagnosis is key and mild symptoms or subtle signs such as meibomian gland expression can point to the need for osmolarity, TBUT, staining and meibography. When things don’t add up, start considering these differential diagnoses. This will allow you to address the patient’s condition more accurately, quickly and, hopefully, lead to a resolution.
Dr. Karpecki is a consultant/advisor to: AMO, Alcon Labs, Allergan, Akorn, Bausch + Lomb/Valeant, BioTissue, Bruder Healthcare, Imprimis, Beaver-Visitec, Cambium Pharmaceuticals, Oculus, Rendia, Eyes4Lives, Focus Laboratories, Katena, Ocusoft, Shire Pharmaceuticals, BlephEx, Science Based Health, Sun Pharmaceuticals, TearLab, TearScience, Topcon, Paragon BioTeck, TelScreen and Visionmetrics.
Dr. Krall is a consultant and advisor to eyeBrain medical.
1. Nichols KK, Nichols JJ, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004 Nov;23(8):762-70 |
