 |
Q:
I have a patient with significant entropion and lashes contacting the globe that are causing a great deal of discomfort. Artificial tears aren’t helping. What are some short- and long-term solutions?A:
There are a number of causes of a lower lid that turns inward. Involutional entropion is established after ruling out cicatricial or mechanical causes, according to Brent Murphy, MD, of Atlanta Oculofacial Plastic Surgeons. “Check the conjunctiva for scarring that is pulling the eyelid inward,” Dr. Murphy says. “Entities such as ocular cicatricial pemphigoid or prior chemical burn can cause this.” Get a good external view of the lids and lashes and gently pull the lower lid down to compare the normal position of the lid with the inverted configuration.
“The short-term solutions you can offer patients with involutional entropion are lubricating ointment and what I like to call ‘the tape trick,’” Dr. Murphy says. Apply a small piece of paper tape vertically on the patient’s cheek to pull the lower lid down enough so that it does not turn in. Apply the tape about a centimeter from the lid margin on the lateral third of the lid. Then apply mild inferolateral tension and secure the tape to the cheek.
“This is a very useful temporary fix that can keep the patient out of trouble while awaiting the definitive fix, which is often surgical,” Dr. Murphy says. “It’s also simple for the patient to reapply at home after getting the tape wet during a shower.”
Involutional entropion is common in people over the age of 60. It is the result of a dehiscence of the lower eyelid retractors and horizontal laxity in the lower eyelid, which causes the lower lid to roll in. When this happens, it can be extremely uncomfortable, and the lashes rubbing the eye can put the cornea at risk of scarring or infection. Lubrication and the tape trick help avoid these problems.
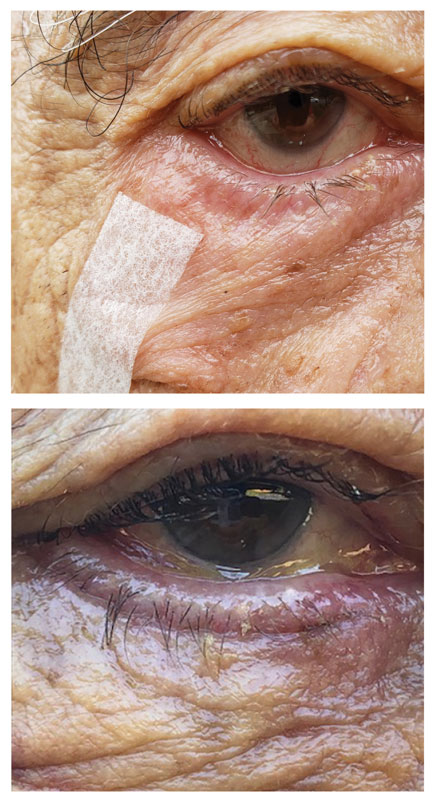 |
| Taping the lid back to its normal position (top) can help resolve an entropion. |
Surgical Options
Surgical repair involves a fairly brief outpatient surgery that corrects the two underlying causes. Dr. Murphy uses the carbon dioxide laser to make an incision in the subciliary crease. Through that incision, the dehisced lower lid retractors can be reattached to the base of the tarsal plate, and a horizontal tightening can be done by full thickness excision of the lateral lid. The lid can then be reattached to Whitnall’s tubercle. The incision is closed with dissolving sutures.
The postoperative course is relatively straightforward, says Dr. Murphy. Cold compresses are used the first three days while the patient is awake, and antibiotic ointment is used on the stitches until they are gone, usually by 10 days. Bruising and swelling dissipate over the first two weeks. Rarely do patients report pain, although the lateral canthal area remains tender for four to six weeks.
“During this time, as well as preoperatively, it is good for the optometrist to monitor the health of the corneal surface,” Dr. Murphy says. Rarely does entropion lead to significant corneal abrasions or ulcerations. “I’ll usually have the patient return four to six weeks after surgery for a final evaluation of the lid,” Dr. Murphy notes.
This surgery provides a long-term fix for entropion, and complications are rare. The most common complication is wound dehiscence in the lateral canthus. “A complete eye examination three to four months after surgery ensures that no refractive changes have occurred from the lid tightening and that the eye is healing as desired,” Dr. Murphy says.
