 |
Q: I send patients out for cataract surgery every month and see all my own post-ops from day one on. Patient after patient comes in not only confused about their three drops, but angry over the price they had to pay for them. Isn’t there a better way?
A: “Every surgeon has their own eye drop regimen for cataract surgery,” says Paul Mitchell, OD, of Eye Care of Delaware. Most regimens consist of three different eye drops: an antibiotic, steroid and NSAID. The out-of-pocket costs can be as much as $500, depending on an individual’s insurance, for surgery in both eyes, says Dr. Mitchell. Compliance is an issue, according to Dr. Mitchell. Often the three drops have different dosing schedules, and the pharmacy may switch to a generic that changes the dosing yet again. The tapering schedule—three drops at different rates over three weeks—can be daunting and confusing, he says.
Dropless Surgery
Some surgeons eliminate the pre- and post-op drop regimens by injecting a compounded mixture of the drugs into the vitreous during surgery, just after intraocular lens (IOL) placement, says Dr. Mitchell.
Two choices exist for the dropless procedure: Trimoxi (intravitreal triamcinolone/moxifloxacin, Imprimis), which contains a steroid and an antibiotic, and TrimoxiVanc, which adds a second antibiotic (vancomycin). The cost of Trimoxi, which is what most use, is around $25. This medication is not covered by insurance, nor can patients be billed for it. Despite the relatively low price per vial, the surgeon or surgery center must bear that cost, which can add up in a high volume practice—a likely reason why more surgeons aren’t using it.
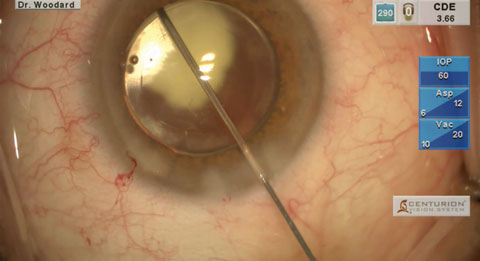 |
| During dropless cataract surgery, a drug mixture is injected into the vitreous, just after IOL placement. |
The injection is performed off-label, since each of its components is approved for other uses. “Patients sign a separate consent for the injection. When given the choice between drops or dropless, they overwhelmingly choose dropless for convenience and cost,” says Dr. Mitchell. “Because the cocktail exists as a white suspension, the vitreous becomes cloudy; the patient may experience hazy vision with floaters,” says Dr. Mitchell. They usually clear within hours, though patients may continue to notice them for a few days, he says.
Contraindications
Glaucoma patients, steroid responders and patients allergic to any component of the injection are not good candidates for the dropless option, says Dr. Mitchell. Patients with small eyes—which can preclude injection—also may not be good candidates, he says. Further, “some surgeons will not do dropless with a toric IOL, because after injecting the medicine, the red reflex through the pupil turns white, making it difficult to see the IOL’s axis markings to ensure it’s on the correct axis,” says Dr. Mitchell.
The potential side effects include: a rise in IOP; blurred or hazy vision for several hours, which usually clears by the next morning; floaters for two to five days; rebound post-op iritis requiring a rescue steroid eye drop, seen days to four weeks after surgery.
“Post-op exams are the same, regardless of which option—drop or dropless—the patients took,” says Dr. Mitchell. “At the one-day post op visit, I like to look in the inferior vitreous with a 90D lens to see how much medicine is in the eye. If little or no triamcinolone is seen, I start the topical steroid that day. If not enough medicine gets in the eye, then a post-op iritis will ensue.”
Another thing to look for is if some of the medicine has migrated into the anterior chamber. “If so, you may see the white triamcinolone on the posterior cornea or in the anterior chamber,” he says. Always make sure to monitor IOP for the first few months after surgery, he says. “A steroid response can occur in some patients, elevating IOP. This can last for three to four months as the steroid dissolves.”
The bottom line: patients save time, money and angst—post-op visits for the OD are made easier—a better experence for all involved.