41st Annual Contact Lens ReportFollow the links below to read the other articles from our 41st annual Contact Lens Report: Corneal Topography for Better Fitting |
Patients diagnosed with corneal ectasia and irregular astigmatism can be a challenge to fit with contact lenses. Options such as soft, conventional corneal gas permeable (GP), hybrid and piggyback contact lenses all come with limitations that stymie success. For example, soft contact lenses may not provide adequate visual acuity, standard GP lenses can decenter or dislodge and the intricacies of piggyback lens systems can be difficult for some patients. In addition, the location or amount of corneal irregularity often makes it impossible to achieve an adequate fit with these contact lenses.
Fortunately, scleral lenses can solve many of these problems. Scleral lenses are large-diameter GP lenses that vault over the cornea and rest on the conjunctiva and sclera. They were the earliest type of contact lenses manufactured and have experienced tremendous growth in recent years.1 Early scleral lenses—manufactured first from blown glass scleral shells and then PMMA materials—were brilliant, but did not work very well.1-3 They caused lens-induced corneal edema due to poor oxygen transmissibility, which led to corneal hypoxia and eventually the discontinuation of lens wear. Additionally, each lens was created by hand and was impossible to replace if lost or broken.1-3
But with today’s improvements and with the right fit, these lenses can help many patients obtain good vision, particularly those with irregular corneas. These fitting tips and tricks will put you on the path to success when fitting scleral lenses for irregular corneas.
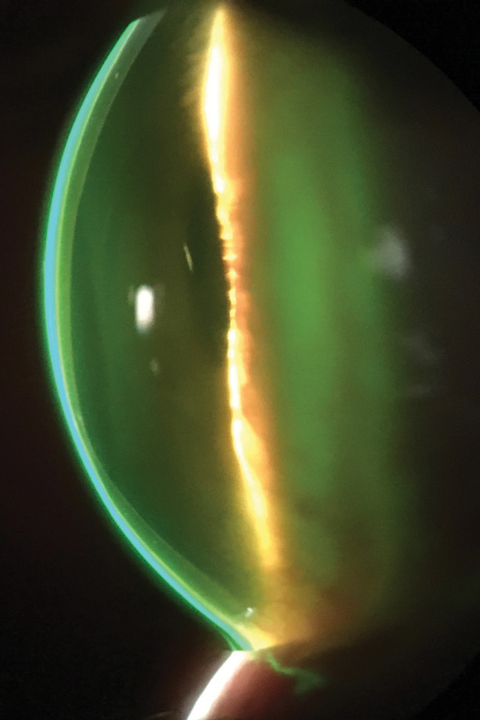 |
| Here is a fluorescein pattern of a scleral lens on an eye with keratoconus. Note complete clearance of the cornea. Photo: John Gelles, OD |
Old Favorite, New Twist
Originally, scleral lenses were prescribed as a last resort and were fit to correct irregular astigmatism due to corneal ectasia and to treat ocular surface disease, including patients with compromised corneas.1-3 Although glass, PMMA and eventually GP scleral lenses were prevalent throughout the first half of the 20th century, the technology and materials available at that time did not ensure reproducibility or clinical success.1-3
Today, better materials, equipment and design reproducibility have overcome many shortcomings. Now, scleral lenses are applied with preservative-free fluid in the post-lens-fluid reservoir. This fluid continuously bathes the ocular surface and corrects for corneal irregularities—improving visual acuity by creating a smooth anterior optical surface.
In 2016, almost 60% of practitioners surveyed reported their use of scleral lenses had increased.4 The role of modern scleral lenses is expanding to include optical correction for both irregular corneas and normal, healthy eyes, as well as for the correction of refractive error and mild to moderate dry eye disease.5
 |
| Protrusion and thinning of the cornea in keratoconus. Photo: John Gelles, OD |
When to Use
There are many indications for scleral lenses for irregular corneas with ectasias, including for keratoconus, keratoglobus and pellucid marginal degeneration.
Primary corneal ectasias include a group of non-inflammatory conditions of the eye distinguished by thinning of the cornea, which results in a distorted corneal surface. Keratoconus is the most common corneal ectasia and causes bilateral asymmetric thinning of the cornea.6 Scleral lenses are particularly beneficial in advanced, notably decentered, keratoconus because they provide lens stability and do not dislodge easily. Scleral lenses cover the entire cornea, providing consistent vision along with good comfort, which can be helpful for patients with keratoglobus, a condition characterized by diffuse thinning and a forward protrusion of the cornea. Custom lens designs that correct corneal irregularities also can provide good vision and comfort for patients with pellucid marginal degeneration, a crescent-shaped band of thinning is present in the peripheral, typically inferior, quadrant of the cornea several millimeters from the limbus.7
In addition, scleral lenses are indicated for secondary corneal ectasias after corneal refractive surgery such as post-LASIK, post-radial keratotomy (RK) and post-penetrating keratoplasty (PK).
Additional indications for scleral lenses are after corneal transplantation and for corneal scars and degenerations or dystrophies such as Salzmann’s nodular degeneration or Terrien’s marginal degeneration. Salzmann’s nodular degeneration is a slowly progressive, typically bilateral, condition characterized by gray-white to bluish nodules near the limbus or in the mid-peripheral cornea.8,9 Terrien’s marginal degeneration produces slowly progressive peripheral thinning of the cornea associated with neovascularization, opacification and lipid deposition. Scleral lenses are particularly helpful for these patients because they correct irregular astigmatism after corneal transplantation, lessen corneal scarring over time, correct corneal irregularities by vaulting over peripheral nodules in Salzmann’s and decrease the amount of corneal neovascularization while continuously bathing the ocular surface during wear.8,9
For corneal scars causing opacity and corneal irregularity along the visual axis, scleral lenses can create a smooth surface and improve vision.6
Due to irregular astigmatism in all conditions, patients are unlikely to achieve adequate vision with spectacles, making a good fit with scleral lenses all the more important.
 |
| This HOA map of an eye with keratoconus shows aberrations beyond sphere and cylinder. While all eyes exhibit some level of HOA, eyes with keratoconus quickly exceed normal levels. Here, the level of higher-order root mean square wavefront error (a typical measure of HOA) is 0.54μm, which is well above the level seen in typical eyes for this pupil size. Image: Jason Marsack, PhD |
In the Literature
Scleral lenses for corneal ectasia have been at the heart of many investigations, most of which suggest these lenses can improve patient’s visual acuity and quality of life. The research also highlights a few issues that might bar scleral lens success.
In one study focused on visual rehabilitation following PK, 28 of 31 patients were successfully fit with scleral lenses, and visual acuity was significantly improved compared with glasses.10 However, the researchers reported 12 graft complications, 10 graft rejections and two cases of microbial keratitis.10
A New Player: CrosslinkingPractitioners should discuss corneal collagen crosslinking with patients with keratoconus. Ideally, in patients with keratoconus and progressive ectatic disease of the cornea, a corneal crosslinking consultation should be performed prior to initiating a contact lens or scleral lens fitting. Although there are no definitive criteria for progression, parameters to evaluate progression include: a change in corneal shape, steepening of the cornea, refraction—including irregular astigmatism—and uncorrected and best-corrected visual acuity. After corneal collagen crosslinking, practitioners can fit patients with scleral lenses. Collaborative care with a corneal specialist will help to determine when a fitting is best. |
In another study of 34 patients (48 eyes) fit with scleral lenses following corneal transplantation, 40% of eyes achieved 20/20 or better with scleral lenses, and 91.7% of eyes achieved 20/40 or better.11 Six eyes developed graft rejection, three of which resumed scleral lens wear following resolution of the rejection episode. There were no cases of associated microbial keratitis.11
Other researchers evaluated scleral lenses in 45 patients (56 eyes) with unacceptable vision after PK.12 All eyes achieved an acceptable fit with scleral lenses, although only 19 patients eventually ordered lenses. The investigators speculate that barriers to completing the process included cost, concerns about lens handling and anticipated delays in receiving lenses. There were no reported cases of graft rejection or microbial keratitis in those who completed the fitting process.12
One study that compared scleral lens fitting with PK in patients with keratoconus found the scleral lens group demonstrated improved visual acuity more rapidly than surgical intervention.13 Data shows more scleral lens patients obtained 20/25 visual acuity or better compared with the PK group. In addition, more complications were observed in the PK group than the scleral lens group.13 Thus, patients with keratoconus who cannot successfully wear other modes of correction can consider scleral lenses before surgical intervention.
Studies also suggest scleral lenses can improve a patient’s quality of life. One study evaluated vision-related quality of life in 30 patients with keratoconus—20 GP lens wearers and 10 non-wearers—and a control group of 30 healthy patients.14 All subscales of the National Eye Institute Visual Function Questionnaire-25 were lower in the patients who had keratoconus. Improved best-corrected visual acuity was achieved in the contact lens group compared with non-wearers.14 Patients who had reduced visual acuity in the better eye had worse distance vision, social functioning, mental health and role difficulties.14 Patients with reduced visual acuity in the worse eye had lower general health scores.14 In keratoconic patients, vision-related quality of life was worse compared with the control group.14 According to this study, a successful contact lens fit that improves visual acuity may improve vision-related quality of life.14
When other researchers evaluated quality of life before and after scleral lens adaptation in patients with keratoconus or after PK, they found quality of life scores of patients wearing scleral lenses were significantly higher compared with those not wearing scleral lenses.15
 |
| Fluorescein pattern of a scleral lens on a post-PK with a protruding graft. Note the increased fluorescein inferiorly. |
A Custom Fit
Keratoconus is by far the greatest indication for scleral lens wear in the published literature, as they correct corneal irregularity due to irregular astigmatism and minimize visual distortion.16-23 Due to their unique fitting characteristics—individualized central and peripheral corneal sagittal depths, front surface and back surface toricity, multifocal optics and diameters—scleral lenses are ideal to provide optical correction in severe forms of corneal ectasia.
Pre-fit testing. Although scleral lenses are fit on sagittal depth, topography or Scheimpflug tomography of the anterior segment are beneficial prior to scleral lens fitting to determine potential areas of concern such as a protruding graft or areas of corneal elevation. Practitioners must evaluate anterior segment health to rule out preexisting staining, corneal microcystic edema or conjunctival elevations. Obtaining horizontal visible iris diameter and evaluating the patient from the side will help to determine how far the cornea protrudes to aid in initial lens selection. Scleral lenses need to vault over the entire cornea, including the highest point. In patients with keratoconus, the location of corneal ectasia is usually the steepest part of cornea, but not always. In some cases, such as post-PK, practitioners should determine endothelial cell count status prior to commencing a scleral lens fitting.
Fitting tips and tricks. The first step to selecting the best scleral lens for a keratoconic eye is to determine the apex of the cornea. If the corneal apex is within the central 4mm of the cornea, a standard geometry lens may achieve a better result. If the corneal apex is outside of the central 4mm, a reverse geometry lens may work better.24,25
In cases of suspected progression, add additional lens clearance (such as 100µm) to avoid corneal touch.24,25
Scleral lenses are known to settle with time. The amount of settling depends on lens characteristics and individual variance and may be up to 200µm.1,4 Wait 20 to 30 minutes at the initial fitting prior to lens evaluation and over-refraction. If needed, incorporate additional sagittal depth for specific lens designs.24,25
Even with ideally fit scleral lenses, at times vision is not as good as expected when fitting patients with keratoconus, and practitioners must consider corneal scarring, lens flexure and correcting higher-order aberrations (HOAs). Although significant central corneal scarring can affect vision, scarring tends to decrease over time with scleral lenses. Practitioners can determine lens flexure with keratometry or topography over the lens and modify the design or add front surface toricity. Also consider reducing lens clearance while avoiding corneal touch or incorporating oblate designs.
Retinoscopy is useful when fitting scleral lenses and especially helpful if HOAs are present. The streak of light with retinoscopy will appear irregular or abnormal, with the possibility of a scissors reflex.24,25
While both corneal and scleral GP lenses can neutralize the irregularity of the front surface of the cornea, irregularity may still exist in the stroma and inferior cornea not managed with standard optical correction. The stability of scleral lenses makes them ideal for the correction of HOAs. For example, one study found HOAs were reduced 65% with corneoscleral lenses in patients with severe irregularity after surgery.26
Adding front surface eccentricity (FSE) to the lens surface may help to improve vision as well.27 The higher the eccentricity value, the more rapid the flattening of the lens from the center toward the periphery.28 Research suggests FSE may compensate for aberrations from the posterior surface, which may counterbalance the poor alignment of the optical axis between the patient and the lens; the eccentricity also may reestablish a prolate surface, thus improving vision.29
With scleral lens FSE correction, investigators found a greater reduction in spherical aberration (86%) compared with lenses without eccentricity correction (66%).28 In 11 eyes with advanced keratoconus corrected with a custom scleral lens with wavefront-guided optics, researchers reported effective correction of HOAs.29 In seven subjects with moderate to severe keratoconus, one study found an improvement of high contrast visual acuity and a reduction of HOAs.30
 |
| These post-PK eyes with ≤700cells/mm2 in the corneal endothelium developed mild corneal edema with fluid-ventilated scleral lenses. Both cases were successful with these fenestrated lenses. Photos: Karen Carrasquillo, OD, PhD |
Following Surgery
Post-PK eyes may have irregular astigmatism and significant graft toricity and decentration, making it difficult to fit corneal lenses. Scleral lenses, by vaulting over the cornea, can be an excellent option for some patients. Still, they come with a few concerns, including graft complications and microbial keratitis.18-20
Pre-fit testing. When fitting a patient after PK, the potential for corneal edema is always a concern. Prior to the fitting, practitioners should evaluate the graft with sodium fluorescein for any pre-existing abnormalities such as microcystic edema or corneal staining. Pre-existing corneal edema is a potential contraindication to scleral lens fitting.6 Careful documentation or photodocumentation is beneficial, and baseline measurements prior to scleral lens fitting will help to identify cornea edema that may arise with scleral lens wear.
Practitioners should also perform pachymetry, along with corneal topography or Scheimpflug tomography of the anterior segment prior to scleral lens fitting to determine the ideal lens design. Every graft is unique, and different designs such as prolate or oblate may be helpful for different eyes. Pachymetry is particularly helpful to check for pre-existing corneal edema. In these cases, challenge the eye with a scleral lens and remeasure pachymetery to determine if additional edema is present.
Reduced endothelial cell count can lead to corneal edema and preclude a patient from successful scleral lens wear. Thus, if there is any concern of a fragile graft, specular microscopy can help to visualize, analyze and document corneal endothelial cells. Normal endothelial cell count is 2,500cells/mm2.31 However, every graft is different. In the adult cornea, the number of endothelial cells decreases with age, stabilizing at around age 50.31 Research suggests practitioners should avoid fitting scleral lenses with an endothelial cell count less than 800cells/mm2.32 To determine scleral lens candidacy, investigators suggest challenging a corneal transplant with scleral lens wear for four to six hours prior to initiating a scleral lens fitting.33 If corneal edema occurs, scleral lenses are contraindicated.
Fitting tips and tricks. It is critical to inform all post-PK patients about the potential for scleral lens wear to exacerbate corneal edema. If a patient experiences hazy vision and sees rainbows around light sources, known as Sattler’s veil, advise the patient to discontinue scleral lens wear immediately, as discontinuing lens wear usually reverses corneal edema. It is important to differentiate Sattler’s veil from post-lens reservoir fogging, which improves with lens removal and reapplication. In addition, front surface scleral lens fogging, unlike Sattler’s veil, improves with cleaning the lens.
Current scleral designs have several parameters clinicians can adjust to help patients avoid corneal edema. Consult with your laboratory to request the thinnest lens possible to prevent corneal edema. To increase tear exchange and help deliver more oxygen to the cornea, reduce the post-lens tear reservoir thickness to a minimum while still avoiding corneal touch, add back surface toricity, change the lens diameter and increase the Dk of the lens to at least 124 or higher.
If corneal edema is still present despite these changes, patients may need to reduce their scleral lens wearing time, add hypertonic sodium chloride or topical steroid drops or use a fenestrated lens. When both eyes have undergone PK, the wearing time may differ between the two eyes of the same patient. Removal and same-day reapplication may help extend wear time for some. It is essential to carefully monitor for early signs of complications and coordinate care with other eye care providers.
Additionally, peripheral curves that are too steep or tight may cause the lens to seal off, and practitioners will have to flatten the peripheral curves to resolve the issue. Likewise, an inadequate limbal clearance may lead to limbal compression and pos-sibly induce corneal edema. Increas-ing the limbal clearance or optic zone diameter could improve the scleral lens fit.
Scleral lenses can be a great option for many irregular cornea patients. With the right pre-fit testing and with a firm understanding of the potential fitting challenges, you can successfully fit most irregular cornea patients with scleral lenses. They can go a long way to improve patients’ quality of life, visual acuity and ocular comfort.
Dr. Barnett is a principal optometrist at the UC Davis Eye Center in Sacramento, Calif. She is a fellow of the American Academy of Optometry, a diplomate of the American Board of Certification in Medical Optometry and a fellow of the British Contact Lens Association.
1. Bowden T. Contact lenses: the story. Kent, United Kingdom: Bower House Publications; 2009. |
