 |
In October, a 65-year-old Caucasian female presented as a new patient. She had moved to the area about one year earlier, and her previous eye care provider, apparently, had followed her closely as a glaucoma suspect and left her with the impression that she was probably going to need medical intervention at some point in the future.
However, upon moving to the area, she felt her new provider had too quickly dismissed her concerns. She came to us for a second opinion.
Presentation
On initial presentation, entering visual acuities were 20/30 OD and 20/25- OS, and best-corrected acuities were 20/20- OU through mildly myopic astigmatic and presbyopic correction. Her pupils were round and reactive to light and accommodation, with no afferent pupillary defect. There was 0.5mm anisocoria that was stable in light and dark.
Her medical regimen included 81mg acetylsalicylic acid QD, and an unknown generic statin and an unknown antihypertensive medication, which she believed was lisinopril. She reported no known allergies to medications.
She had no family history of glaucoma, but reported her older sister has macular degeneration.
Evaluation
A slit lamp examination of her anterior segments was completely unremarkable. There was fine SPK noted centrally following instillation of anesthetic and fluorescein, but otherwise all was normal. Angles were judged to be wide open at the slit lamp. Applanation tensions were 20mm Hg OD and 19mm Hg OS at 10:45am. Central corneal thickness measurements were 531µm OD and 542µm OS. Threshold 24-2 visual fields were relatively clear, but with non-contiguous defects in the arcuate areas in both eyes, and reliability indices were moderate at best.
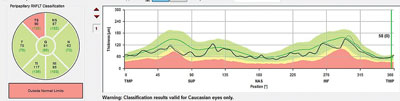 | |
| Note the TSNIT and global optic nerve sector analysis of a patient similar to the one discussed in this column. There is depression of the superior temporal RNFL of enough substance to be reflected in the corresponding global optic nerve sector as aberrant. Smaller RNFL defects would be seen on the RNFL TSNIT scan, but might not show up on the sector analysis. In that case, the entire sector analysis would be erroneously flagged as normal. |
Through dilated pupils, her crystalline lenses were characterized by mild anterior cortical and nuclear cataracts, with vacuoles in both eyes. There were bilateral posterior vitreous separations.
Stereoscopic evaluation of her optic nerves demonstrated average-sized discs with a cup-to-disc ratio of 0.55 x 0.70 OD and 0.55 x 0.65 OS. The superior temporal neuroretinal rim of each disc was somewhat thinned. There appeared to be an NFL wedge defect in the superior temporal region of the RNFL in the right eye extending to the disc. The retinal vasculature was characterized by mild arteriolar sclerotic retinopathy in both eyes. Both maculae were characterized by fine RPE mottling, with no evidence of subretinal neovascularization. There was a small ERM perifoveally in her left eye. Her peripheral retinal evaluations were unremarkable in both eyes.
Multimodal 30 degree and 55 degree imaging of both posterior poles was obtained which readily showed the ERM in her left eye, as well as a well-defined RNFL wedge defect superior temporally in her right eye.
OCT imaging was also obtained for both eyes. The TSNIT graph for her right eye demonstrated a depression in the area of the wedge defect, but was otherwise normal, and that of the left eye was essentially normal in the double hump appearance. Global indices of the optic nerve and RNFL scans were normal in both eyes, as were the macular thickness maps centered on the ETDRS grid.
Discussion
After the initial examination, I discussed with the patient my concerns that she did, in fact, have glaucoma in the right eye—primarily manifest as the NFL defect extending to the optic nerve—and that she was a suspect in the left eye. She was rather articulate in her questioning as to why, specifically, I felt she had glaucoma and more so as to why I felt the best course of action would be medical intervention for her right eye.
Unless there are compelling reasons to do so, I prefer not to medicate a new patient who has glaucoma at the first visit. This mostly has to do with fostering a feel for diurnal variations and developing a stronger doctor/patient relationship.
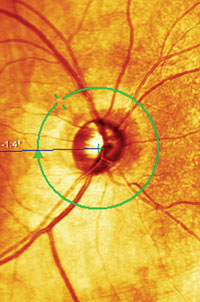 | |
| This image shows a wedge defect in the RNFL, a similar condition to that of the patient in this case. |
Accordingly, at the completion of the initial examination, I asked to see her back in approximately a month to obtain several other measurements, in particular a HEP FDF visual field, HRT-3 optic nerve imaging and another IOP reading.
During the discussion, the patient posed an awkward question about the clinical capabilities of the clinician who, she felt, dismissed her situation. As I have mentioned before in this column, it serves no purpose to disparage another practitioner, especially when the encounter is painted through the articulation of the patient. In situations like these, I simply fall back on the fact that each clinician is different, and while we may be looking at the same disease, we look at it through different experiences and clinical intuitions.
Follow-up
When the patient returned for follow-up, her IOPs were 22mm Hg OD and 20mm Hg OS. FDF field testing did reveal an arcuate defect inferiorly in her right eye, consistent with the RNFL defect, and HRT-3 imaging correlated well with the clinical appearance of the optic nerve. I had also obtained a copy of her medical records at the patient’s request.
In reviewing her previous records, and in particular the OCT, I saw what may have been a deciding piece of information for the previous clinician in calling the patient normal—a lack of “red disease.” All indices on the earlier OCT scan were flagged as “green” which is what our eyes tend to gravitate toward when we evaluate optic nerve and retinal scans.
Red Disease
In earlier columns, I discussed the issue of “red disease;” that is, when a doctor looks at a particular instrument’s normative database for an assessment of whether or not disease is present. The unfortunate impact of having normative databases is in the quick clinical assessment of the patient when either red or green shows up, implying either the presence or absence of disease.
It is incredibly important to realize that normative databases are simply statistical representations of the patient population used to gather the normative data. In other words, the normative database looks at a typical bell curve distribution of a particular index, concentrating on the center of the bell curve. As we all know, there are always outliers that are, frankly, normal. Just because a database may flag a particular index as red does not necessarily mean disease is present. Conversely, if a normative database flags a study as green, that does not mean no disease is present.
In looking at the earlier OCT, as well as the current OCT, the macular thickness maps were all “normal” (read as green). The RNFL scan was also green.
Perhaps the previous provider quickly glanced at the scans and saw all green and quickly determined that the patient was fine. I don’t know, but that is certainly a possibility.
We noted an RNFL defect, but a normal appearance in the global RNFL scan data and macular scans, similar to the scan provided on page 77. That pertains to a significant enough wedge defect to skew the data of the entire sector. In this patient’s case, the wedge defect was small and not of enough substance to affect the whole sector of the RNFL scan.
And therein lies the main crux of this case: statistics do not a disease make, nor do they absolve one from disease.