Optical coherence tomography (OCT) has evolved over the last several years from a device used in only a few practices to one found in many primary eye care clinics. The technological growth in ocular imaging has allowed for profound advancements in the clinician’s ability to recognize subtle abnormalities, differentiate stability from progression in ocular pathology and identify disease stages.
Clinicians have four prominent commercially available spectral-domain (SD) OCT models to choose from: Spectralis SD-OCT (Heidelberg Engineering), 3D OCT-2000 (Topcon Medical Systems), Avanti RTVue XR (Optovue), and Cirrus HD SD-OCT 5000 (Carl Zeiss Meditec). This article outlines the basics of OCT imaging and walks you through how to analyze retinal nerve fiber layer (RNFL) thickness, macular thickness and ganglion cell complex using each model.
| Table 1. Comparison of Four Commercially Available SD-OCT Models | ||||
| Model (Manufacturer) | Cirrus HD-OCT 5000 (Carl Zeiss Meditec)2 | 3D OCT-2000 (Topcon Medical Systems)5 | Spectralis SD-OCT (Heidelberg Engineering)6 | Avanti RTVue XR (Optovue)7 |
| Scanning Speed (A-scans per second) | 27,000-68,000* | 27,000 | 40,000 | 70,000 |
| Axial Resolution (μm in tissue) | 5 | 5-6 (longitudinal) | 3.9 (optical) | 5 (depth) |
| Minimum Pupil Diameter (mm) | 2 | >2.5 | 2.5 | 2.5 |
| Focus Adjustment (diopters) | +20 to -20 (internal) | +12 to -13 (in fundus photo) | +24 to -24 | +20 to -15 |
| *Cirrus OCT (5000 model with version 6.5 software) acquires 68,000 scans per second with fundus photos | ||||
OCT Basics
While the earliest time-domain (TD) OCT technology could only acquire 400 scans per second, current SD-OCT models, depending on the manufacturer, can capture between 26,000 and 70,000 axial-scans per second (Table 1).1,2 This improvement is beneficial to the clinician because it minimizes image artifacts, makes 3D imaging possible and increases image resolution.1,3
Today’s SD-OCT can also provide an axial resolution of 3µm to 6µm within tissues, compared with previous TD-OCT technology, which had a maximum resolution of 10µm.3,4 The increased speed and resolution provide an enhanced ability to visualize retinal layers.
With eye tracking capability and image registration, artifacts are much less common than in prior technology. These models also have increased fundus camera resolution and focus options for detailed image capture compared with prior TD-OCT (Table 2). OCT’s ability to define particular layers of the retina, known as “segmentation,” as well as depth localization in tissue, also aids in identifying points of interest within the scans. Two more benefits of new OCT software are 3D reconstruction of the retinal image and structural comparison functions, which compare a lesion within an area of the OCT image to the associated location visible on a retinal photograph. Current models allow image acquisition with miotic pupils, which is advantageous for patients who struggle with dilation due to age or other factors.
| Table 2. Comparison of Imaging Modes and Capabilities by Model | ||||
| Cirrus HD-OCT 50002 | 3D OCT-20005 | Spectralis SD-OCT6 | Avanti RTVue XR7 | |
| Imaging Modes | SD-OCT, confocal scanning laser ophthalmoscope (cSLO) | SD-OCT, near IR color fundus photos | SD-OCT, IR fundus photo with cSLO | SD-OCT |
| Fundus Photos Scanning Modes | IR | Color, FA, FAF, red-free | IR, blue laser FAF, red-free photos, FA, ICG angiography, panning camera | Live IR |
| Image Field of View | Fundus photo, 36x30 degrees | Fundus photo, 30-degree digital zoom | Fundus photo, 30x30 degrees (optional 55 degree lens) | OCT, 40 degree wide-field reference scan |
OCT Models
The Cirrus HD-OCT’s current software features additional layouts that enable the clinician to see nerve and macular findings on a single printout and formulate functional and structural relationships between visual fields and OCT data, respectively.3 An upcoming software algorithm is expected to add a widefield analysis of the posterior pole, including the optic nerve head (ONH), RNFL and ganglion cell analysis (GCA), in one printout.3
The 3D OCT-2000 uses a high resolution, 16.2 megapixel fundus camera as well as a color touchscreen.5 The software provides the clinician with same-time image viewing of the fundus photo and OCT. The software also locates the OCT line scan in the fundus photo for easy comparison between imaging modalities.5
The Spectralis SD-OCT’s imaging modalities include fluorescein angiography (FA), red-free images, indocyanine green (ICG) angiography, infrared photography and ultra-widefield angiography. The new OCT2 module is an upgrade option that offers a 70,000Hz to 85,000Hz scan rate.6
The Avanti RTVue XR software has motion correction and can evaluate multiple layers of the peripheral retina simultaneously. Alternative models available to the clinician include the iVue, which is a more compact instrument. It has similar specifications as its larger counterpart, but may be beneficial to doctors who need to use the device in multiple practice locations or outside the office, as in nursing home care.7
All instruments possess a retinal thickness scanning mode as well as an optic nerve and RNFL acquisition and analysis (Table 3). All OCT models allow for the change of the size, length and width of the line scans, depending on the pathology imaged. Current OCT systems also possess recognition software and progression or change functions to accurately track and monitor progression over time based on each model’s normative data (Table 4).
| Table 3. Scan Acquisition and Analyzing Options by Model | ||||
| Model | Cirrus HD-OCT 50002 | 3D OCT-20005 | Spectralis SD-OCT6 | Avanti RTVue XR7 |
| Scanning Range | Retina/nerve, anterior segment | Retina/nerve, anterior segment | Retina/nerve | Retina/nerve, cornea, angle |
| Scan Acquisition: Macula | Macular cube (512x128, 200x200), HD five-line raster | 3D scan, radial scan, seven-line raster scan | Line, star, volume | 3D cube (320x320), widefield imaging (12mmx9mm), line, HD-line, crossline, HD-crossline 3D macula, radial slices, multiple patterns |
| Scan Acquisition: Nerve | Optic disc cube (200x200) | 3D scan, circle scan | Circle, volume | RNFL 3.45 |
| Scan Acquisition: Anterior Segment | Five-line raster, cornea, manual angle | Radial corneal scan, line angle scan | Not on standard model | Cornea line, cornea crossline, angle, raster, 3D cornea |
| Posterior Segment Analysis | Macula: macular thickness, macular change, ganglion cell, RPE change Nerve: RNFL thickness, guided progression 3D imaging | Glaucoma and macula report (12mmx9mm wide scan) Macula: 3D macula report, macular drusen analysis Nerve: 3D disc report, RNFL trend analysis, glaucoma analysis | Macula: Real time, fast, dense, detail, posterior pole, seven lines Nerve: Fast, dense, posterior pole, nerve head circle | Widefield enface mapping Combined RNFL and ganglion cell change report Macula: Retinal trend analysis, ganglion cell complex, retinal overview report, multilayers enface report Nerve: Retinal nerve fiber and optic disc, optic disc structure analysis |
| Anterior Segment Analysis | Cornea: Manual thickness Angle: Manual angle measurement | Cornea: Thickness map, curvature and radius Angle: Manual angle measurement | Not on standard model | Cornea: Corneal power, pachymetry map, epithelium thickness map Angle: Automated measurement |
SD-OCT Limitations
Recent literature suggests that, although reproducible OCT findings are common among healthy individuals, variable results can occur when retinal pathology is present due to the differences in acquisition and boundary identification between machines.8-11
Along with variability in retinal presentations, clinicians can encounter ambiguous findings of non-glaucomatous optic neuropathies and normal optic nerve anatomy, which can lead to false positive and false negative OCT results. Researchers have determined that nerve diameters greater than 4.0mm2 can falsely affect the accuracy of nerve fiber analysis results.3,12 Accuracy is also limited by high refractive error and axial length. Longer eyes can artificially cause thinner peripapillary retinal nerve fiber layer (pRNFL) measurements, while shorter eyes may falsely represent higher pRNFL values due to camera magnification.13
Repeatability of RNFL and retinal thickness measurements over time must also be considered when monitoring for progression of an ocular disease state. Researchers determined that SD-OCT has an inter-visit tolerance limit of 95% for average pRNFL—equivalent to approximately 4µm.14 Cross sectional studies suggest a normal age-related decline of RNFL is 0.2µm per year, and the rate of decline may be higher in eyes with greater baseline retinal nerve fiber layer thickness.13,15 These considerations must be taken into account when evaluating OCT data and managing progressive ocular conditions.
Studies suggest that clinicians should be cautious when comparing thickness measurements from one brand of OCT with another in the same generation due to differences in algorithm acquisitions between machines.14,16 This often leads to a difficult decision for a provider looking to make a change from an OCT model of one company to another company’s when baseline data has already been obtained on established patients.
| Table 4. Comparison of SD-OCT Normative Databases by Manufacturer for US Models | ||||
| Model | Carl Zeiss Meditec1 | Topcon Medical Systems2 | Heidelberg Engineering3 | Optovue4 |
| Number of Subjects | 284 | 182 | 201 | 480 |
| Ages (years) | 19 to 84 | 19 to 84 | 18 to 78 | 18 to 84 |
| Gender (M/F) | 133 M 149 F | Disc: 54 M / 92 F Macula: 112 F / 61 M | 111 M 90 F | N/A |
| Ethnicity | 43% Caucasian 24% Asian 18% African American 12% Hispanic 1% Indian 6% Mixed Ethnicity | 64% Caucasian 21% African American 15% Hispanic | Caucasian | 33% Caucasian 22% Asian 20% African American 12% Hispanics 12% Indian 1% Other |
| Anatomy Evaluated | pRNFL thickness Optic nerve Parameters GCL + IPL thickness Macular thickness | Optic disc Macula | RNFL thickness | RNFL thickness Ganglion cell complex Macular thickness |
| Study Location(s) | United States, China | United States | Germany | 11 Clinical sites worldwide |
| 1. Carl Zeiss Meditec I. Cirrus HD-OCT 2015. 2. Inc. T. Topcon 3D OCT Series Normative Database. Available from: www.topconmedical.com. 3. Engineering H. Spectralis HRA+OCT 510(k) Summary. Available from: www.accessdata.fda.gov/cdrh_docs/pdf12/K121993.pdf. 4. Optivue I. 510(k) Summary Optovue, Inc. RTVue with Normative Database. Available from: www.accessdata.fda.gov/cdrh_docs/pdf10/K101505.pdf. | ||||
Although SD-OCT technology gives highly reproducible results in optimal patients, the technology can still be confounded by poor signal strength. Common causes include media opacity, ocular surface disease, reduced tear film quality, miotic pupils and image or motion artifacts. Software algorithm errors, including improper identification of anatomical boundaries and scan misalignment, can lead to decreased reliability and repeatability in testing.17,18 Poor patient cooperation secondary to ocular saccades, blink artifacts and conditions such as tremors and nystagmus can result in poor image capture, even by a seasoned operator.
| Common OCT Abbreviations and Terminology A-Scan/B-Scan: Axial images allowing for 3D representation/line scan of longitudinal images Deviation Map: Graph comparing patients’ deviation to normative age-matched database EDTRS: Early Treatment Diabetic Retinopathy Study En face OCT: View of retina or optic nerve as a clinician would view during funduscopy GCL/GCA/GCC: Ganglion cell layer/ganglion cell analysis/ganglion cell complex GCL-IPL: Ganglion cell layer-inner plexiform layer Line Scan: Scan through a tissue which can be adjusted to orientation ONH: Optic nerve head Raster: Scan generally consisting of five lines that can have various spacing and orientation (customizable) RNFL/pRNFL: Retinal nerve fiber layer/peripapillary retinal nerve fiber layer SD-OCT: Spectral-domain optical coherence tomography Thickness Map: Graph comparing retinal thickness to normative age-matched database Tomogram: A two-dimensional image of a slice through a tissue (i.e., retinal tissue) TSNIT: Linear graph of concentric nerve fiber layer thickness in respect to normative database Volume Scan: 3D representation formed from the vertical & horizontal line scans, representing a block or cube of retinal tissue |
Despite these variables, OCTs are a valuable tool in clinical practice, especially given the limitations of other, more subjective ocular ancillary tests. For example, fundus photography can have low inter-observer agreement, especially when evaluating diffuse retinal nerve fiber loss. Alternatively, in visual field testing, reduced reliability can occur due to the subjectivity of the patient’s responses. Also, the sensitivity of visual field testing in diagnosing early disease processes needs to be considered, as significant retinal ganglion cell (RGC) loss often occurs before visual field defects are evident.19
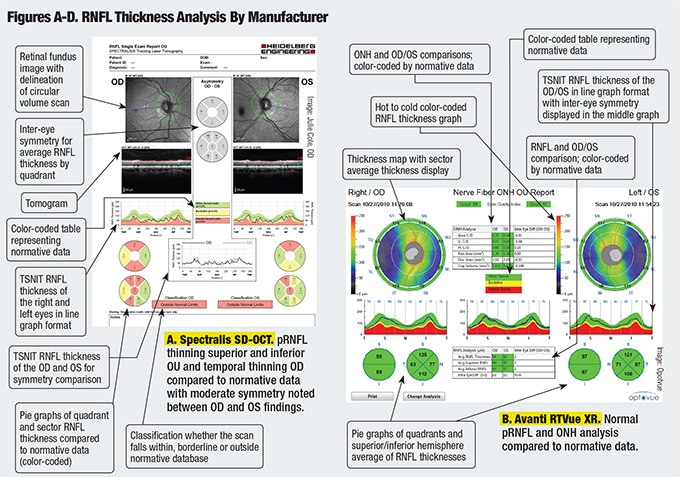
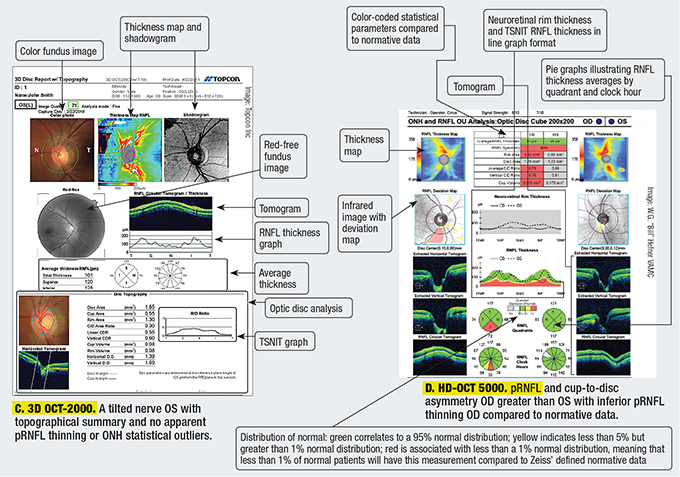
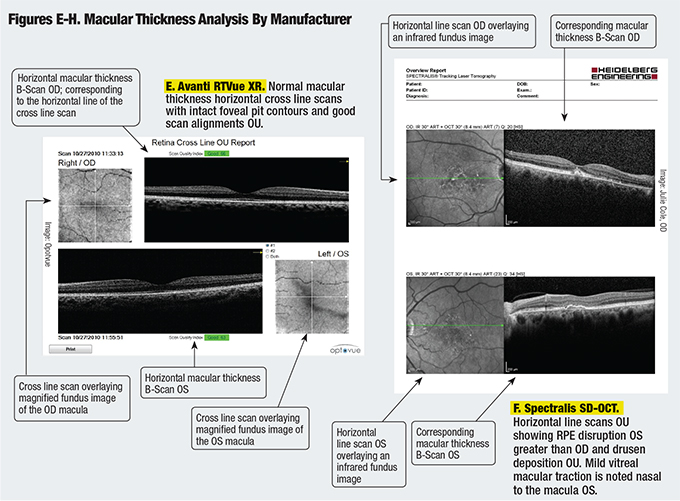
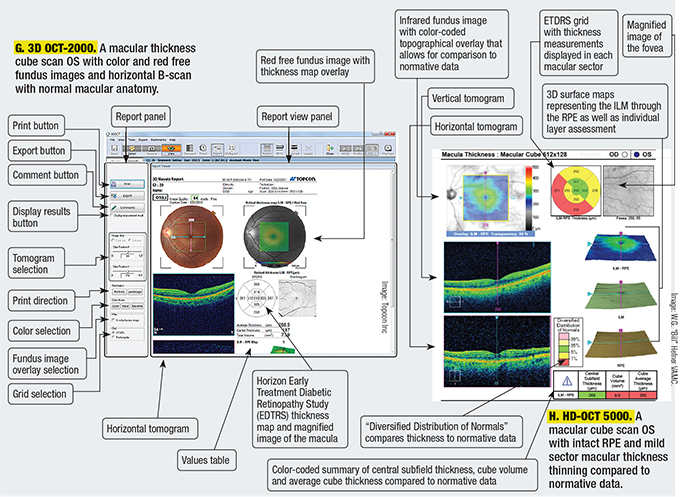
Comparing OCT Scans
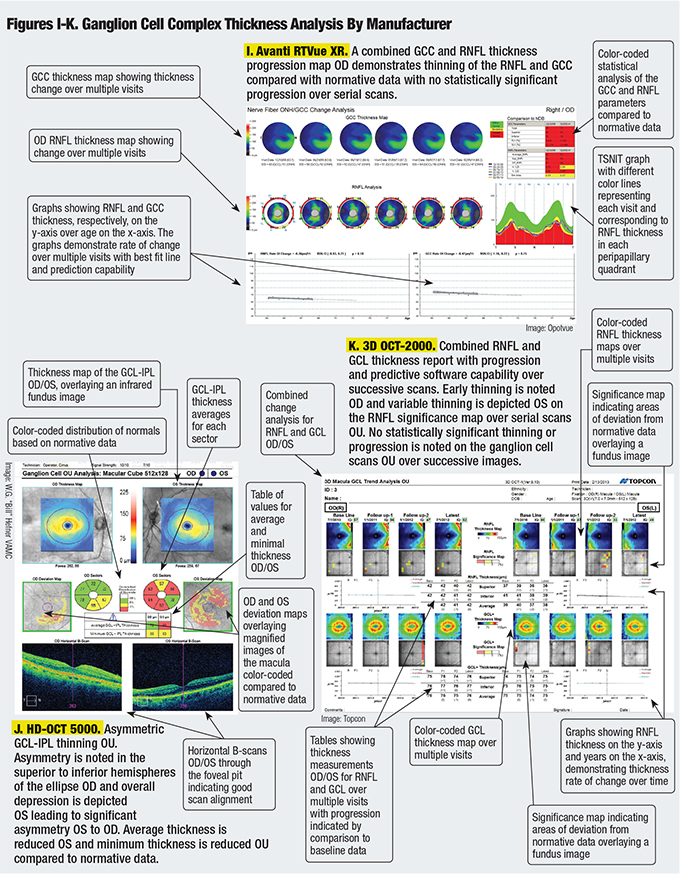
While all four SD-OCT models are comparable in many ways, each one presents the information differently. Figures A-K are comparisons of RNFL thickness analysis, macular thickness analysis and ganglion cell complex analysis as represented by each model.
The Future of OCT
A significant challenge with OCT technology is keeping up with advances without losing previous data during system and software upgrades. Clinicians may have to establish an entirely new baseline when transferring care to a newer model OCT—a challenge clinicians faced with the transition from TD-OCT to SD-OCT. Time will tell if swept source (SS) OCT technology, the newest iteration, will lead to similar consequences.
SS-OCT has improved acquisition speed, volume and depth of ocular tissue measurements compared with SD-OCT technology.2 This technology has the potential to provide excellent image resolution from the posterior hyaloid face through the choroid without the need for multiple image averaging or loss of internal retinal layer image quality when viewing deeper retinal or choroidal structures, as is the case of enhanced depth imaging functions with SD-OCT. The first commercially available SS-OCT, the DRI OCT Triton (Topcon Europe Medical BV) has a scan speed of 100,000 A-scans per second and uses a 1050nm wavelength to pass through cataracts and retinal hemorrhages.20
OCT has also been adapted to surgical suites for intraoperative use, and portable models have been incorporated into neonatal ophthalmologic care.21 Handheld OCT models have been used for screening purposes in primary care settings to evaluate potential pathologies of the eye, ear and skin.22
OCT is also being used in cardiology, dermatology and respiratory medicine, and is under investigation as a possible tool to monitor cancer progression and response to therapeutic intervention.23-26
The combination of Doppler and OCT—referred to as phase variable OCT—and other similar technologies collectively referred to as OCT-angiography (OCT-A), can give a representation of retinal blood flow and provides the ability to define capillary networks in tissue.2 The advantage of OCT-A is that no dye injection is needed, which eliminates the risk of allergic or adverse reactions and provides more visible capillary plexuses.27 Additionally, it is not impeded by dye leakage as compared to FA testing.27 The technology also can provide a 3D image of the retina and choroid, visualizing superficial and deep vessels, which is an advantage compared to FA and ICG imaging.28
The future of OCT may lie in the coupling of other imaging modalities with OCT to better evaluate structures at a molecular level.2 The continually evolving nature of OCT technology has made it a crucial and integral part of early diagnosis of ocular disease, as well as a reliable and noninvasive way to identify disease progression. We look forward to future advancements that will augment and refine our use of OCT technology in the primary eye care setting.
  |
  |
 |
Drs. Mazzarella and Cole are staff optometrists at the W.G. “Bill” Hefner VAMC in Salisbury, NC.
2. Drexler W, Liu M, Kumar A, et al. Optical coherence tomography today: speed, contrast, and multimodality. Journal of biomedical optics. 2014;19(7):071412.
3. Carl Zeiss Meditec I. Cirrus HD-OCT. Available from: www.zeiss.com/meditec/en_us/products-.
4. Kotowski J, Wollstein G, Folio LS, et al. Clinical use of OCT in assessing glaucoma progression. Ophthalmic surgery, lasers & imaging: the official journal of the International Society for Imaging in the Eye. 2011;42 Suppl:S6-14.
5. Topcon I. 3D OCT-2000 Spectral Domain OCT. Available from: www.topconmedical.com/products/3doct2000.htm.
6. Engineering H. Spectralis: Multi-modality diagnostic imaging of the eye. Available from: www.heidelbergengineering.com/us/products/spectralis-models/.
7. Optivue I. Optovue. Available from: http://optovue.com.
8. Terasaki H, Shirasawa M, Yamashita T, et al. Comparison of foveal microstructure imaging with different spectral domain optical coherence tomography machines. Ophthalmology. 2012;119(11):2319-27.
9. Branchini L, Regatieri CV, Flores-Moreno I, et al. Reproducibility of choroidal thickness measurements across three spectral domain optical coherence tomography systems. Ophthalmology. 2012;119(1):119-23.
10. Bressler SB, Edwards AR, Chalam KV, et al. Reproducibility of spectral-domain optical coherence tomography retinal thickness measurements and conversion to equivalent time-domain metrics in diabetic macular edema. JAMA Ophthalmol. 2014;132(9):1113-22.
11. Suzuma K, Yamada Y, Liu M, et al. Comparing central retinal thickness in diabetic macular edema measured by two different spectral-domain optical coherence tomography devices. Japanese Journal of Ophthalmology. 2011;55(6):620-4.
12. Mansoori T, Balakrishna N, Viswanath K. Influence of disc area on retinal nerve fiber layer thickness measurement by spectral domain optical coherence tomography. Indian Journal of Ophthalmology. 2014;62(5):615-8.
13. Knight OJ, Girkin CA, Budenz DL, et al. Effect of race, age, and axial length on optic nerve head parameters and retinal nerve fiber layer thickness measured by Cirrus HD-OCT. Archives of Ophthalmology. 2012;130(3):312-8.
14. Mwanza JC, Chang RT, Budenz DL, et al. Reproducibility of peripapillary retinal nerve fiber layer thickness and optic nerve head parameters measured with cirrus HD-OCT in glaucomatous eyes. Invest Ophthalmol Vis Sci. 2010;51(11):5724-30.
15. Leung CK, Yu M, Weinreb RN, et al. Retinal nerve fiber layer imaging with spectral-domain optical coherence tomography: a prospective analysis of age-related loss. Ophthalmology. 2012;119(4):731-7.
16. Leite MT, Rao HL, Zangwill LM, et al. Comparison of the diagnostic accuracies of the Spectralis, Cirrus, and RTVue optical coherence tomography devices in glaucoma. Ophthalmology. 2011;118(7):1334-9.
17. Chhablani J, Krishnan T, Sethi V, Kozak I. Artifacts in optical coherence tomography. Saudi Journal of Ophthalmology: official journal of the Saudi Ophthalmological Society. 2014;28(2):81-7.
18. Darma S, Kok PH, van den Berg TJ, et al. Optical density filters modeling media opacities cause decreased SD-OCT retinal layer thickness measurements with inter- and intra-individual variation. Acta Ophthalmologica. 2014.
19. Spaeth GL, Reddy SC. Imaging of the optic disk in caring for patients with glaucoma: ophthalmoscopy and photography remain the gold standard. Survey of Ophthalmology. 2014;59(4):454-8.
20. Medical TE. Dri OCT Triton Swept Source Optical Coherence Tomography. Available from: www.sweptsourceoct.eu.
21. Maldonado RS, Izatt JA, Sarin N, et al. Optimizing hand-held spectral domain optical coherence tomography imaging for neonates, infants, and children. Invest Ophthalmol Vis Sci. 2010;51(5):2678-85.
22. Shelton RL, Jung W, Sayegh SI, et al. Optical coherence tomography for advanced screening in the primary care office. J Biophotonics. 2014;7(7):525-33.
23. Yonetsu T, Bouma BE, Kato K, et al. Optical coherence tomography-15 years in cardiology. Circ J. 2013;77(8):1933-40.
24. Sattler E, Kastle R, Welzel J. Optical coherence tomography in dermatology. Journal of Biomedical Optics. 2013;18(6):061224.
25. Hariri LP, Villiger M, Applegate MB, et al. Seeing beyond the bronchoscope to increase the diagnostic yield of bronchoscopic biopsy. Am J Respir Crit Care Med. 2013;187(2):125-9.
26. Vakoc BJ, Fukumura D, Jain RK, Bouma BE. Cancer imaging by optical coherence tomography: preclinical progress and clinical potential. Nat Rev Cancer. 2012;12(5):363-8.
27. Nagiel A, Sadda SR, Sarraf D. A promising future for optical coherence tomography angiography. JAMA Ophthalmol. 2015;133(6):629-30.
28. Spaide RF, Klancnik JM Jr., Cooney MJ. Retinal vascular layers in macular telangiectasia type 2 imaged by optical coherence tomographic angiography. JAMA Ophthalmol. 2015;133(1):66-73.
