 A 64-year-old Hispanic female
presented for an evaluation
at the request of her primary
care physician. She reported
her vision had been blurry for the
past several months and further
described the problem as a steady,
painless, progressive loss of vision.
Additionally, she noted a foreign
body sensation––as if there were
grains of sand in her eyes. Her last
eye examination was approximately
four years earlier.
A 64-year-old Hispanic female
presented for an evaluation
at the request of her primary
care physician. She reported
her vision had been blurry for the
past several months and further
described the problem as a steady,
painless, progressive loss of vision.
Additionally, she noted a foreign
body sensation––as if there were
grains of sand in her eyes. Her last
eye examination was approximately
four years earlier.
She has a history of severe rheumatoid arthritis (RA) and currently is using several medications, including 10mg prednisolone QD and 200mg hydroxychloroquine BID.
Her best-corrected visual acuity measured 20/30 OU. Her pupils were equally round and reactive to light, with no evidence of afferent defect. Confrontation visual fields were full to careful finger counting OU, and ocular motility testing was normal. Her Amsler grid results were normal OU.
The anterior segment was significant for 1+ diffuse injection and moderate central corneal staining in both eyes. Further, we documented grade 1-2+ posterior subcapsular cataracts in both eyes. Intraocular pressure measured 14mm Hg OU.
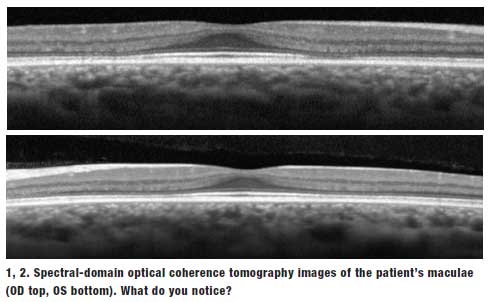
Her optic nerves appeared healthy on dilated fundus examination, with a small cup and good rim coloration and perfusion OU. The vessels were of a normal caliber and her peripheral retinae were unremarkable. We performed a spectral-domain optical coherence tomography scan, which is available for review (Figures 1 and 2).
Take the Retina Quiz
-
What additional testing should
be recommended for our patient?
- Amsler grid.
- Color vision.
- 10-2 threshold visual field.
- All of the above.
-
How would you interpret the
spectral-domain optical coherence
tomography (SD-OCT) images of
our patient's maculae?
- Normal.
- Focal defect at the level of the ganglion cell layer.
- Diffuse macular edema.
- Focal loss at the level of the inner segment/outer segment (IS/OS) junction.
-
What do the findings in our
patient represent?
- Hydroxychloroquine-induced toxicity.
- Fabry disease.
- Epiretinal membrane with diffuse macular thickening.
- None of the above.
-
What is considered to be a safe
dose for hydroxychloroquine?
- 7.5mg/kg.
- 6.5mg/kg.
- 5.0mg/kg.
- Both b and c are correct.
Discussion
Our patient is suffering from moderate dry eye, as well as posterior subcapsular cataracts. The cataracts likely are due to long-term prednisone use.
The patient explained that she has been taking 400mg Plaquenil (hydroxychloroquine, Sanofi-Aventis) for approximately 15 years. Careful clinical evaluation of both maculae appeared normal.
So, based on clinical evidence, can we conclude that she doesn't have hydroxychlorine-induced macular toxicity? Indeed not! Further testing is indicated, including a 10-2 visual fields evaluation, as well as any one of the following: SD-OCT, fundus autofluorescence (FAF) or multifocal electroretinogram (mERG). We chose to order an SD-OCT scan, and instructed her to return within a few weeks for a scheduled 10-2 visual field.
Her SD-OCT scan was quite revealing. In the outer retinal layers at the level of the IS/OS junction, we noted a focal loss or defect on the nasal and temporal side of the right macula. The left macula exhibited a similar presentation, but the line was not as bold and probably represented diffuse loss. Given these findings, our patient likely has early hydroxychloroquine-induced macular toxicity.
Hydroxychloroquine is a member of the quinolone family of drugs. Rheumatologists frequently prescribe the agent to treat RA, systemic/ discoid lupus erythematosus and other connective tissue and inflammatory disorders. Chloroquine and, to a lesser extent, hydroxychloroquine are well known to cause macular toxicity. In later disease stages, affected individuals may manifest a "bull's eye" macular legion with a corresponding visual field defect. Unfortunately, once these changes are actually visible in a clinical evaluation, the toxicity is already fairly advanced.
With the advent of SD-OCT and other specialized tests, such as FAF and mERG, eye care providers now can detect these changes before they affect visual function. With such advanced diagnostic technologies in mind, Michael F. Marmor, MD, and associates published revised recommendations for screening patients on Plaquenil therapy in 2011.1 The updated guidelines removed color vision testing and Amsler grid as acceptable screening methods, and instead recommended that patients be followed with 10-2 visual fields and at least one of the following advanced diagnostic tests: mERG, SD-OCT or FAF.1
All patients who are started on hydroxychloroquine should undergo a baseline eye exam within the first year of treatment. This should include a dilated fundus evaluation, 10-2 white-on-white threshold visual fields and at least one of the aforementioned advanced tests. These examinations do not have to be repeated for at least five years after dosing initiation, unless the patient exhibits other risk factors for hydroxychloroquine-induced macular toxicity.
Retinal toxicity from Plaquenil occurs in approximately 0.5% to 2.0% of long-term users; however, the true risk may be higher, because those percentages are derived from short-term use studies.1,2 A dose of 6.5mg/kg/day in a person of "ideal body weight" is believed to be a safe dosage.1 For example, a patient who weighs 135lbs should take two 200mg tablets per day (61.2kg x 6.5mg/kg/d = 398mg/d).1,2
Dr. Marmor and associates recently published research evaluating the risk of associated toxicity from long-term Plaquenil use.2 They conducted a retrospective study of an integrated health organization consisting of 3.4 million members. Of this population, approximately 2,361 patients used hydroxychloroquine for at least five years. The overall prevalence of toxicity was 7.5%, but this number varied based on daily dosage and duration of use.
Of interest, they used "real body weight" to calculate the daily dosage compared to "ideal body weight." When using real body weight, the researchers determined that 5.0mg/kg/day was equivalent to the ideal body weight measurements of 6.5 mg/kg/day. Using these calculations, Dr. Marmor's group determined that for a dosage of 4.0mg/ kg/day to 5.0mg/kg/day, the prevalence of macular toxicity dropped to less than 2% within the first 10 years and rose to almost 20% after 20 years.2 They concluded that when Plaquenil is taken at dosages greater than 5.0mg/kg/day, the risk of retinal toxicity is two to three times higher.2
Our patient weighed approximately 130lbs. Using Dr. Marmor's "real body weight" calculation: 130lbs = 58kg x 5.0mg/kg/d = 290mg. Thus, her daily dose of Plaquenil should be approximately 290mg, not 400mg as prescribed. So, it's no wonder she developed retinal toxicity after 15 years of use.
We informed her rheumatologist that she developed retinal toxicity from the hydroxychloroquine use. We then educated the patient about her cataracts, but explained that she was not yet ready for surgery. Additionally, we started her on Restasis (cyclosporine, Allergan) BID and Lotemax (loteprednol, Bausch + Lomb) BID for her dry eye.
She returned two weeks later for a 10-2 visual field and, indeed, it showed a classic circular paracentral scotoma in both eyes that did not involve central fixation. After informing her rheumatologist of these findings, she was instructed to discontinue hydroxychloroquine therapy.
1. Marmor MF, Kellner U, Lai TY. Revised recommendations on screening for chloroquine and hydroxychloroquine retinopathy. Ophthalmology. 2011 Feb;118(2):415-22.
2. Melles RB, Marmor MF. The risk of toxic retinopathy in patients on long-term hydroxychloroquine therapy. JAMA Ophthalmol. 2014 Oct 2. [Epub ahead of print]
