Expanding the scope of practice for optometrists in the United States is an ongoing process made difficult by the fact that the profession is legislated on a state-by-state basis. Yet, especially over the last decade, many states have been successful in passing legislation that extends practice privileges of optometrists, which, in turn, is improving access to care. The American Optometric Association (AOA) reports that 99% of the US population has access to a doctor of optometry, meaning that the passage of these bills could allow hundreds of thousands of people to access potentially vision-saving treatment without having to travel far from their homes or see a different doctor.1 However, only four states (Alaska, Kentucky, Louisiana and Oklahoma) currently allow optometrists to perform every procedure outlined in their education and training.2
 |
| To date, six states allow optometrists to use SLT to lower intraocular pressure in glaucoma patients (Oklahoma, Kentucky, Louisiana, Alaska, Arkansas and Wyoming). Click image to enlarge. |
It wasn’t until 1971 that Rhode Island became the first to authorize the use of diagnostic drugs, followed by West Virginia and North Carolina, before which optometrists had little elbow room to do much other than visual field testing.3 Fast forward to today and more and more states are allowing optometrists to perform laser and minor procedures, administer various injections, prescribe a growing number of medications and controlled substances and manage more patients independently without having to consult with or refer patients to an ophthalmologist.
Glaucoma management is one category of patient care that has strongly benefited from expansion laws. As of 2021, every state in the country can treat glaucoma topically. In addition, seven states are now allowed to perform at least one type of laser procedure (Oklahoma, Kentucky, Louisiana, Alaska, Arkansas, Mississippi and Wyoming).
“The reason why more states are granting optometrists authority to perform different procedures is twofold: the first is that the knowledge, education and training of optometry reflects that they should have the authority in their scope of practice to provide those services to their patients, and the other is the safety history modeled by previous practice changes,” says Nebraska’s Christopher Wolfe, OD, chair of the AOA State Government Relations Committee.
“Glaucoma management has been in the profession for 20, 30 years or longer in some states,” notes Dr. Wolfe. “It’s difficult for someone to say ODs are not managing glaucoma appropriately and not trained on it. The same sort of thing is happening with other procedures; we can offer patients care through safe procedures that are much more accessible.” Dr. Wolfe also points out that the way licensure laws are written is an important part of ensuring ODs will be able to use new medications and treatment options in patient care when they become available.
“For example, suppose a law states that you can treat glaucoma with a beta-blocker. If a different medication like prostaglandin comes around, then you wouldn’t have access to that new medication that’s been around for 20 years and is safer and less of a treatment burden for the patient, and you might be going back to the legislature to battle for that,” Dr. Wolfe explains. “Rather, what the law might say is to allow for the treatment of glaucoma. That way, any new medication that comes around relative to the treatment of glaucoma would then be available to physicians and to their patients.”
Expanding privileges not only allows optometrists to use the training and skills they are already capable of, but it also lets ODs care for more patients in-office, offer a wider variety of treatment options and, consequently, improve the vision and eye health of more people. Let’s explore some of the scope expansion bills that have passed over the last two decades and how they’re being implemented in the practice of optometry across the states.
Hands-on Optometry: Newcomers Aplenty
In just the last three years, eight states mounted legislative efforts to expand scope for their ODs—and most succeeded. Many of these next-gen laws allow optometrists to manipulate ocular structures directly, bringing invasive surgical procedures—e.g., intralesional steroid injection, curettage, foreign body removal, selective laser trabeculoplasty (SLT) and YAG capsulotomy—to optometry.
Uncle Sam Favors Scope LawsThe federal government showed its support of expanded practice laws with the release of a 2018 report titled Reforming America’s Healthcare System Through Choice and Competition. The document, advocating the rights of non-medical clinicians such as optometrists, included the following guidelines: (1) allow clinicians to practice at the “top of their license,” (2) allow non-physicians to be paid directly and (3) eliminate supervision requirements between physicians and “care extenders” (like ODs).The report also covered the potential of telehealth, regarding technology as a way to increase competition and accessibility, even across state lines. It states that telehealth is most effective when it replicates in-person care, evaluates conditions using digital images and allows for quicker information acquisition than would be possible with in-person visits. AOA Applauds Report Calling for States to Improve Safe Patient Access to Critical Eye Health Services. AOA. December 12, 2018. www.aoa.org/about-the-aoa/press-room/press-releases/report-calls-on-states-to-review-scope-laws?sso=y. Accessed September 21, 2021. |
Arkansas. One defining battle of the current scope era took place here two years ago. The state changed its definition of optometry—literally—in March 2019 with the passage of HB 1251, which had been reworked following its initial rejection a month prior. The practice of optometry in Arkansas now encompasses some minor ophthalmic surgeries, including procedures of the lid, adnexa or visual system, as well as the use of ophthalmic lasers (making it the fifth state to do so).
Before the bill passed, ODs in Arkansas were not allowed to perform any procedure that required anything other than a topical anesthetic, and, according to the president of the Arkansas Optometric Association, Joe Sugg, OD, the road to changing that legislation was anything but smooth.
“The challenges we faced from our opposition were truly relentless and unprecedented,” Dr. Sugg recalls. “Every step of the way, we faced the well-funded and organized efforts from medicine and ophthalmology, under the name ‘Safe Surgery Arkansas.’ The group even challenged the scope law after it was signed by the governor and began collecting signatures to place the new law on the November 2020 general election ballot,” he says. Partly because most of the collected signatures turned out to be unqualified canvassers, a petition granted in favor of optometry was able to push the act forward. Since it went into effect, the benefits of the bill for both practices and patients have been made apparent.
“A friend and colleague of mine in another rural practice had a glaucoma patient who was left debilitated by a stroke and could no longer walk to the office or instill his eye drops,” Dr. Sugg shares. “This OD arranged transportation for the patient to come to the office and performed SLT on him, helping save his vision. These are the types of stories about the care we optometrists provide in our offices that our opposition takes for granted, but fortunately more and more state legislatures are understanding how beneficial these expanded scope laws can be for our patients.”
Maryland. In March 2020, an exciting scope of practice law (HB 447/SB 447) went into effect here, giving optometrists more prescribing authority and removing several requirements for ophthalmology referrals. ODs in the Old Line State are finally permitted to prescribe most topical agents and oral pharmaceuticals. They also no longer have to refer patients to an ophthalmologist for open-angle glaucoma treatment, corneal and conjunctival foreign body removal or to order labs, cultures or blood tests.
Vermont. In a rare loss, the Office of Professional Regulation under Vermont’s Secretary of State decided in late January 2020 that it would not allow optometrists in the state to perform the advanced procedures being proposed by the Vermont Optometric Association (VOA), including various forms of laser treatment and injections. This jurisdiction came despite several states having recently passed similar scope of practice expansion laws for ODs (Oklahoma, Kentucky, Alaska and Louisiana).
As justification for opposing the law, the state referred to a JAMA Ophthalmology 2016 report that suggested the incidence of repeat laser trabeculoplasty procedures doubles when done by an optometrist rather than an ophthalmologist; however, critics point out that the study has several limitations and does not provide a sound argument for depriving Vermont ODs of expanded practice privileges. The growing and successful track record of scope of practice laws in the United States also demonstrates the great potential of the proposed legislation, which will surely not be the VOA’s last effort to advocate for ODs and their patients.
Iowa. In June 2020, the House passed a bill allowing Iowa optometrists to treat certain ocular conditions with injections. HF 310 gave the state’s ODs the right to administer subconjunctival injections to treat ocular conditions, intralesional injections to treat chalazia, botulinum toxin (including for cosmetic purposes) and injections to counteract an anaphylactic reaction. While newer OD graduates will have the education and clinical training required to administer these injections, the Iowa Optometric Association (IOA) is offering workshops for those needing to acquire the new skillset, and even offered one prior to the bill’s passage to prepare the state’s ODs for what was to come.
In order for a licensed OD in Iowa to begin using these injections, the state’s board of optometry put forward the following training requirements:
- Complete 24 hours of approved educational training pertaining to injections.
- At least four of the 24 hours must be clinical training, and at least five of the 24 hours must address administration and side effects of injection treatment for botulinum toxin and chalazia.
Brian Kirschling, OD, who served as IOA’s president from April 2020-2021, says that the bill passed the House three times in the years leading up to 2020 and received widespread bipartisan support, but the COVID-19 pandemic did temporarily take top priority at the House. He notes that despite it being a long process, building relationships with state legislators is a crucial part of advocating for increased practice privileges that will expand access to care across the state population.
“After three or four years, I think some people start to think, ‘Well, this is never going to happen,’” Dr. Kirschling says. “Then, to have [the bill pass], despite the fact that COVID was an immediate priority for everybody in the world, is a testament to not only that sweat equity and financial support in those relationships, but also a testament to the respect for optometry in the state of Iowa.”
Dr. Kirschling says the IOA has upcoming workshops scheduled for the start of 2022 to allow more optometrists in the state to complete the training necessary to begin administering the injections. While this bill will certainly allow more of Iowa’s residents to access critical care without having to travel far, he explains that the efforts will be ongoing for scope of practice expansion.
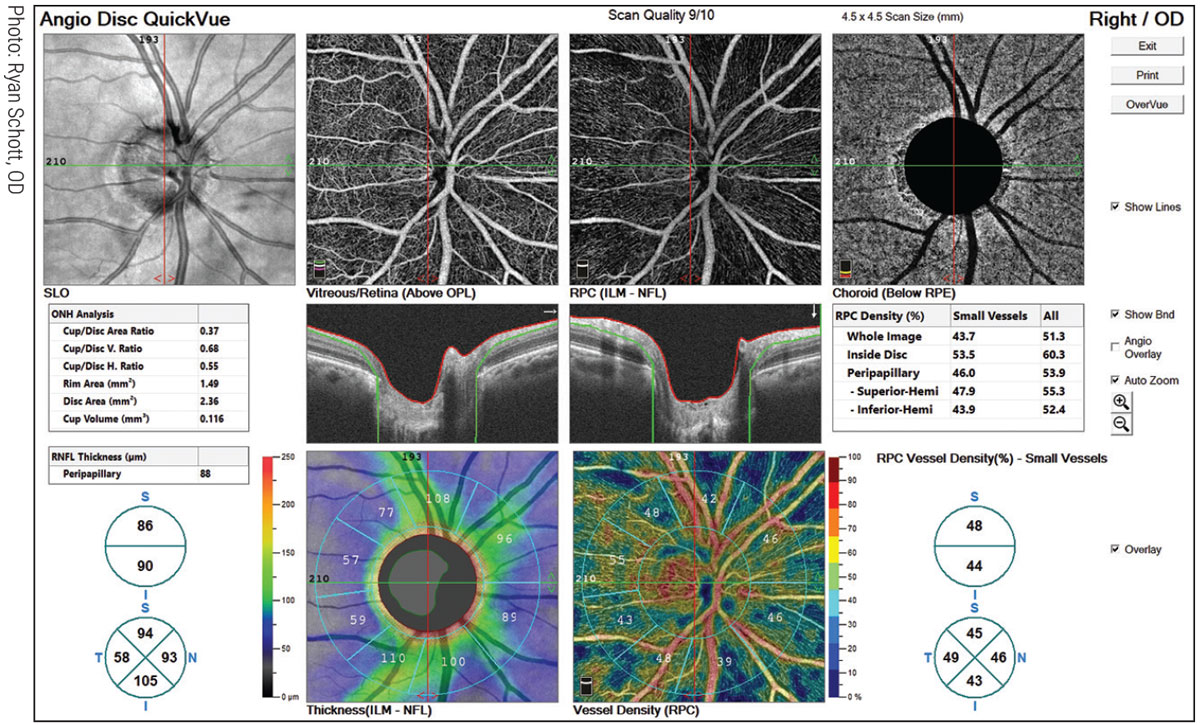 |
| It was only this past summer that all 50 states achieved autonomy in glaucoma care when a Texas law freed ODs there from having to comanage all aspects with an MD. Above: an AngioVue OCT-A scan identifies capillary dropout that corresponds to RNFL dropout. Click image to enlarge. |
“You can never sit back and rest on your laurels for too long; you have got to think: how do we how remain an attractive state for young people to want to practice in, and how do we provide the best care for the most Iowans across the state?” says Dr. Kirschling. Some counties have only one or two eyecare providers for the entire region, he notes, and “chances are that it’s going to be an optometrist in large portions of Iowa.” As a result, “it’s very important that when new procedures or medications become available, we’re always making sure that we are included in those discussions and thinking about how to provide access to care for the vast majority of the state population,” he says.
Pennsylvania. For the first time in 18 years, the Keystone State expanded the scope of practice for optometrists in October 2020 when Gov. Tom Wolf signed HB 2561, an amendment to the state’s Optometric Practice and Licensure Act first passed in 1980. Among other new privileges, the amendment gives ODs much more authority to examine, diagnose and treat patients in-office by removing restrictions such as the requirement for the secretary of health to approve medications before doctors write a prescription. The bill grants the state’s board of optometry the exclusive right to manage and determine the optometric formulary, meaning patients will have access to needed medications sooner and more conveniently.
Mississippi. This past spring, Mississippi passed a law that now allows its optometrists to prescribe oral steroids and use certain injectable agents, including local anesthesia in some procedures, as well as permits them to excise and remove chalazia and non-cancerous growths in and around the eyelid. The bill was approved by Gov. Tate Reeves in March 2021, prior to which, it was amended to allow for any OD credentialed by the state board to perform laser capsulotomy procedures.
“We are proud to be one of the first states to be able to perform these types of procedures, and we are very grateful for the states that came before us,” says Ryan Wally, OD, legislative chair of the Mississippi Optometric Association. “We have had people from Louisiana, Arkansas, Oklahoma and Kentucky all reach out to us to help us with our efforts. If I had one piece of advice for other states going forward, I would encourage them to reach out to the states that have been successful, because the advice and expertise they can offer is valuable.”
Dr. Wally explains that for ODs in Mississippi to be able to perform the added procedures and start prescribing oral steroids, they must first complete mandated training, including a continuing education (CE) course and an eight-hour preceptorship with an ophthalmologist or licensed, credentialed optometrist, followed by a state board exam and clinical skills assessment, during which the OD must perform a laser capsulotomy procedure.
“We already have almost 150 optometrists statewide who are credentialed in these procedures. As soon as the bill passed, our state board went to work to begin that process,” says Dr. Wally. “[The practice expansion] has really helped with access to care and being able to offer excellent eye care statewide.”
 |
| Lesion removal is one procedure being added to practice scope in a growing number of states that gives patients quicker access to care with the ability to be treated in-office. Above: excision of a squamous papilloma in an optometric office. Photo: Jackie Burress, OD, Rodney Bendure, OD, and Lisa Kedzuf, OD. Click image to enlarge. |
Wyoming. Only a few weeks after Mississippi’s bill passed, optometrists in Wyoming received their big win when Gov. Mark Gordon signed the scope expansion bill, HB 39, on April 2 of this year. The state’s ODs, practicing in 22 of 23 counties, can now perform YAG laser capsulotomy, SLT, laser iridotomy and lesion removal, as well as enjoying more prescribing authority. The last scope of practice update for Wyoming ODs was 26 years ago in 1995, highlighting the significant need for this legislation that better aligns practice rights with current education and training.
Kari Cline, executive director of the Wyoming Optometric Association (WOA), says that Wyoming ODs must complete certain CE courses and a period of proctoring to be able to perform the specific procedures. “I would say about 95% of practicing optometrists in the state of Wyoming have completed those courses,” she says. Ms. Cline notes that a lot of the graduating students are coming out of school with training in the new procedures and may only need to take a refresher course depending on the skills and education they received.
Dana Day, OD, past president and current legislative chair of the WOA, says that optometrists and their patients alike in Wyoming are excited about the services they can now offer in-office. “I was able to present the option to a couple of my patients recently to have their laser procedures done in the office or have them referred to another practicing physician, and they were excited to be able to just stay here and have it done in our office when they used to have to go somewhere else,” says Dr. Day.
He continues, “Our optometrists are excited; as you can see, 95% of them, or close to that, have already done the certification and are looking forward to incorporating these expanded privileges into their practices for the betterment of patient care.” Dr. Day encourages any ODs in Wyoming who haven’t yet taken the certification to do so and embrace the new opportunities.
Texas. The Lone Star State was the lone hold-out on independent glaucoma care until this past June, when Gov. Greg Abbott signed SB 993, giving ODs in the state the authority to manage most forms of glaucoma independently without the requirement of comanagement with an ophthalmologist. With the exception of Schedule I and II controlled substances, Texas ODs can also now treat eye conditions with oral meds.
“This bill is not only great for optometrists, but ophthalmologists too,” says Houston’s Jill Autry, OD. “Many patients would never even see an eye doctor if they had to find an ophthalmology office. As optometry becomes more medical, more medical issues are found, and many are going to need to be referred to ophthalmology. As people look at optometrists as their primary eye care physicians, it’s not only patients and optometrists that gain, but ophthalmologists, primary-care practitioners (PCPs), endocrinologists and rheumatologists—I think it’s really better for everybody.”
Now that ODs in Texas can prescribe antivirals, patients could avoid negative outcomes from conditions that otherwise may not be treated in time due to barriers to access of the drug, Dr. Autry explains. “Antivirals are pretty commonly used to treat ocular disease. The alternatives are very expensive, and many times are not readily available at pharmacies. Oftentimes, you really need to start those antivirals within 24 to 72 hours, and by the time you get the patient in to see an ophthalmologist or their PCP, visual outcomes may suffer.” Thankfully, patients seeking critical antiviral treatment in Texas will no longer need to go to such lengths.
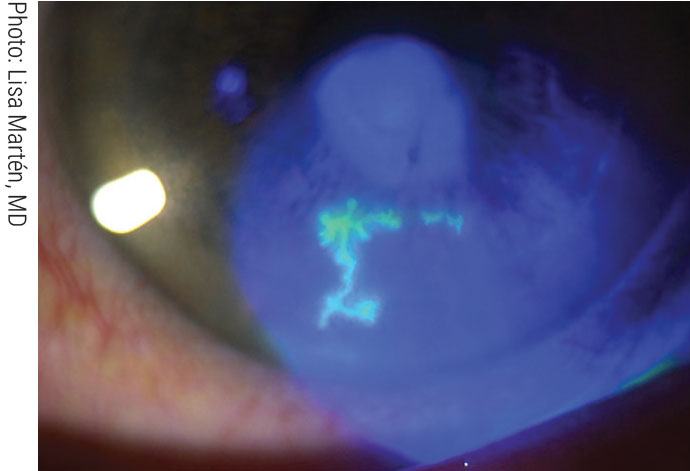 |
| As antivirals can be hard to access, giving ODs the authority to prescribe them helps reach more patients in need. Click image to enlarge. |
The state’s board of optometry did not mandate specific training for ODs to begin taking advantage of the expanded privileges since the law went into effect on September 1, but there are CE courses for those who wish to learn about the various medications they may now be prescribing to their patients. Dr. Autry says that Texas ODs would love to eventually be able to perform laser and surgical procedures like a growing number of states around them, but negotiations in this recent bill may prevent that from happening for at least the next several years.
Next-Gen Scope Veterans
Let’s check in with some of the early success stories in the current wave of hands-on optometric procedure laws to see if their experiences may point the way toward what to expect for the roll-outs now happening in more recently updated states.
“Optometrists have been very pleased with the laws that allow them to practice full scope and they end up working more effectively with their ophthalmology colleagues/surgeons because of the clearly defined areas of practice scope,” notes Kentucky’s Paul Karpecki, OD, a longtime champion of optometric scope expansion and greater involvement in medical care. “The specialists are seeing more appropriate patients that need to be in their office and optometry is seeing the primary care patients that need to be monitored for diabetic retinopathy or glaucoma, as examples.”
Michigan. The last adjustment to Michigan’s scope of practice for optometrists happened back in late 2002 with the signing of HB 5552, coined the “Therapeutic Care Legislation.” The bill’s passage meant ODs were no longer required to consult with an ophthalmologist prior to treating glaucoma, allowing for speedier treatment and a more seamless process for both physicians and patients.
The legislation also granted Michigan ODs the right to prescribe oral drugs, including Schedule III, IV and V controlled narcotic substances. Since then, the scope of practice in Michigan has been at a standstill but continues to be monitored, says Jeff Towns, executive director of the Michigan Optometric Association.
“We have a lot of frustrated recent graduates in the state that really aren’t able to practice the scope of optometry they are being taught and trained to provide, which unfortunately means a lot of our graduates are leaving the state for others that allow them to practice at a level commensurate with their training and education,” says Towns. “In a way, Michigan taxpayers are helping to pay for the education and training of doctors who are going to apply that training outside the borders of our state. Like any state, we need to be looking to the future.”
Because of the nature of the work, it’s easier for optometrists than it is for ophthalmologists to practice successfully in less populated and rural areas of a state, notes Towns. He says that while the demand for eye care is growing as the population increases, “We need to look at who is the most likely provider to help meet that demand, and optometrists are in a perfect spot to do that.”
Oklahoma. Optometrists in this southern state have been performing laser procedures since 1998, practicing in the first state permitting them to do so with one of the best scope of practice laws in the country. Six years later in October 2004, Gov. Brad Henry signed a rule that also made it the only state at the time allowing optometrists to perform over 100 types of surgeries, including those using a scalpel. The regulation gave ODs the ability to cut the eyelid or eye surface to remove cancer lesions, administer medication via injections in the center of the eye and inject Botox around the eye. Since no other states’ ODs at the time were allowed to perform such delicate procedures, the rule was met with controversy initially; however, as years pass and states nationwide are implementing similar laws, the safety history and benefits of optometrists performing these procedures can hardly be disputed.
Big Retailers Fight BackIn 2018 in Oklahoma, large retail chains, primarily Walmart, began to fight against prescription eyewear being sold in their stores and allowing optometrists to open practices in commercial settings. Public voters ruled in favor of the retailers when questioned about the matter in a ballot question in the 2018 midterm elections. However, Walmart and the Oklahoma Association of Optometric Physicians ended up agreeing on a compromise: ODs could offer independent eye care services and prescription eyewear within retail facilities, so long as it is a separate legal entity owned and operated by the OD. The legislation was amended twice and eventually approved by Gov. Kevin Stitt in May 2019. |
Kentucky. In February 2011, Kentucky joined Oklahoma as only the second state at the time allowing optometrists to perform laser procedures when the Better Access to Quality Eye Care bill (SB 110) was signed into law by Gov. Steve Beshear with bipartisan support. The bill allows optometrists to use the most current methods of drug administration, including certain injections and drug-dispensing contact lenses, as well as perform minor surgical procedures to correct ocular abnormalities.
While the training for these procedures is built into the curriculum for today’s optometry students, the bill requires all ODs who haven’t already to complete necessary training and certification requirements before performing each class of procedures.
This past summer, the Bluegrass State also conferred onto the state’s optometrists the right to dispense pharmaceutical agents in-office.
Dr. Karpecki, who practices in Lexington, notes that “the overarching issue is that, other than in some major metropolitan cities, there is a severe shortage of ophthalmologists, resulting in optometry having to provide greater patient access and in-office services.”
Indiana. On January 1, 2014, the scope of practice expanded for Indiana optometrists when the state lifted the prohibition against ODs performing injections. A more recent law that passed in 2020 also added Indiana optometrists to the list of providers authorized to engage in telemedicine and issue prescriptions to patients over the phone, a practice privilege being granted to ODs in an increasing number of states around the country, especially following the intense demand for telemedicine brought on by the COVID-19 pandemic.
Nebraska. In May 2014, the state’s Better Access to Quality Eye Care bill was signed into law by Gov. Dave Heineman. The legislation lifted former restrictions and gave optometrists the ability to prescribe several oral drugs including steroids, glaucoma medications and immunosuppressives. It also authorized potentially life-saving injections that treat anaphylaxis.
Because such a large portion of the state is rural, extending prescribing authority for ODs has afforded many Nebraskans the opportunity to receive certain treatments in-office, as opposed to jumping through hoops to access care that patients may desperately want or need, notes Dr. Wolfe, who also serves as the legislative chair for the Nebraska Optometric Association.
“Since 1998, when ODs in Nebraska were first allowed to begin treating and managing glaucoma, no complaints have been sent to the board, nor have any actions had to be made relating to the treatment and management of glaucoma or expanded authority, which really speaks to the safety of the profession for providing those services to patients,” says Dr. Wolfe. He adds that no additional training was required for ODs to begin administering care based on the updated regulations of the 2014 bill since every optometrist in the state with a therapeutic license has been trained and tested on these medications since the early 1990s.
Louisiana. Gov. Bobby Jindal signed HB 1065 in June 2014 permitting Louisiana optometrists to perform various ophthalmic procedures including YAG laser capsulotomy and laser peripheral iridotomy. The bill, initially met with controversy after a similar effort was shot down the year before, also began allowing ODs in the state to prescribe Schedule III drugs. The legislation made Louisiana the third state in the country to allow ODs to use lasers.
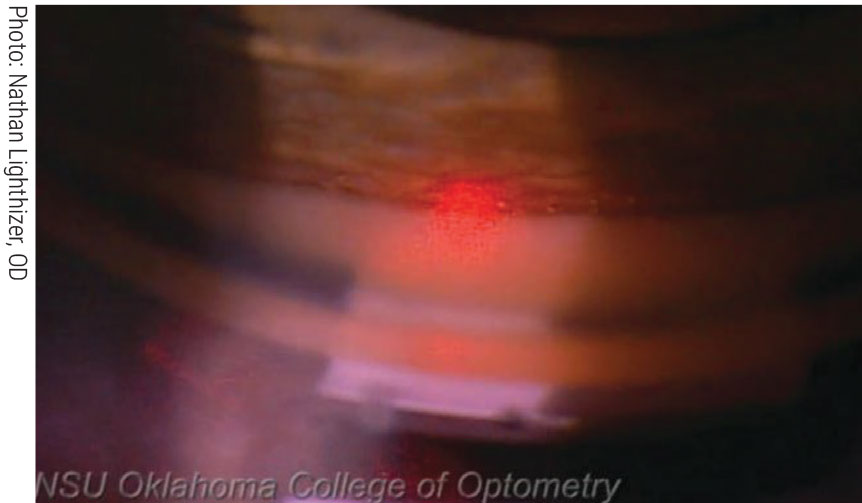
 |
| Today, capsulotomies can be performed in optometry offices in seven states. Oklahoma was the first state to authorize ODs to do so. At left, Oklahoma’s Nathan Lighthizer, OD, prepares to treat a patient. At right, we see the resulting central clearance postoperatively. Click image to enlarge. |
Alaska. Optometrists in The Last Frontier had reason to celebrate in July 2017 when the “Optometry and Optometrists” bill (HB 103) was signed into law by Gov. Bill Walker, giving the Alaska Board of Examiners in Optometry the authority to write regulations that allow the state’s ODs to practice everything they’ve been taught in optometry school, including use lasers and perform surgical procedures. Alaska is the largest state in the country, yet also ranks fourth in states with the lowest population. In a region where people and communities are so dispersed, giving optometrists more practice privileges makes treatment accessible for thousands of Alaskans who may not have been able to access it before.
Virginia. In spring 2018, Virginia enacted SB 511, authorizing optometrists to administer limited injections of Schedule IV steroids for chalazia treatment. Prior to the law that went into effect on July 1, 2018, ODs in the Old Dominion State could only prescribe Schedule II hydrocodone combination products (hydrocodone plus acetaminophen) and Schedules III and IV controlled substances and devices. The new law requires that optometrists in the state pass certain training requirements and be board and TPA certified to be able to administer steroid injections.
Final Thoughts
Scope of practice in the field of optometry in the United States is moving in a positive and exciting direction for doctors, healthcare workers, patients and communities, especially those in less populated areas of the country. The more people who have their eyes examined regularly and consider optometrists their primary eye care providers, the more diseases and instances of vision loss or blindness that may be prevented.
The bottom line: there are more cataract surgeries than there are surgeons, notes Dr. Karpecki, leaving an underserved patient base for minor procedures, advanced treatments like SLT, YAGs and iridotomy lasers.
“We still need to work with ophthalmology for surgical procedures and tertiary care—and in some cases, secondary care—but aside from that, optometry can manage most ophthalmic conditions and needs to stay educated and aware of them."
1. The scope of success. AOA Focus. August 9, 2021. https://www.aoa.org/news/advocacy/state-advocacy/the-scope-of-success?sso=y. Accessed September 21, 2021. 2. Optometrist scope of practice. National Conference of State Legislatures. March 31, 2021. https://www.ncsl.org/research/health/optometrist-scope-of-practice.aspx. Accessed September 21, 2021. 3. Cooper SL. 1971-2011: forty-year history of scope expansion into medical eye care. Journal of the AOA online. March 23, 2012. https://newsfromaoa.wordpress.com/2012/03/23/1971-2011-forty-year-history-of-scope-expansion-into-medical-eye-care. Accessed September 21, 2021. |
