 |
Q:
I just got my DEA registration renewal—for $731! I wrote two pain med Rxs last year. Is it worth it?
A:
Having recently gone through a scope of practice battle in his home state, Ben Casella, OD, of Augusta, Ga., is more mindful than ever of how hard optometry’s predecessors fought to obtain the privileges some assume have always existed. “It takes tremendous efforts just to be able to practice what we are taught as optometrists,” says Dr. Casella, immediate past president of the Georgia Optometric Association. “Every prescription we write is possible because of giants in our profession who fought for the privilege—and it is a privilege,” he says.
 |
| Pain meds can be vital when needed, as in this instance of trauma. |
Practitioners need to be ready for any patient that comes into the office. Narcotic analgesics have a definite role in primary eye care and are critical to treating a patient in distress. “Eye pain can mean severe pain, especially related to the cornea,” says Dr. Casella. “So, when I get the call at 9pm on a Friday for a large fingernail abrasion, my DEA license is my insurance policy—it ensures I am able to treat that patient to the best of my ability and get them through the night and weekend.”
If a bandage contact lens alone doesn’t alleviate the patient, narcotic analgesics may be indicated. Since these medications work through the central nervous system to elevate one’s pain threshold—thus altering the perception of pain—their peak effect occurs around two hours after ingestion, says Dr. Casella. “It’s important to educate the patient that a pill will not have the immediate effect that a drop of proparacaine or a bandage contact lens may,” he says. Patients need to stay ahead of the pain and not wait to dose.
It’s important to remember that a full day of treatment with the maximum recommended dosage of an oral NSAID approaches the analgesic effect of a narcotic. Dr. Casella points out that, of course, most hydrocodone narcotics that ODs prescribe are combined with either acetaminophen or an NSAID. Be alert to any additional over-the-counter analgesics the patient is taking so you can calculate combined dosages. Topical NSAIDs can take the edge off, but typically won’t provide enough relief on their own.
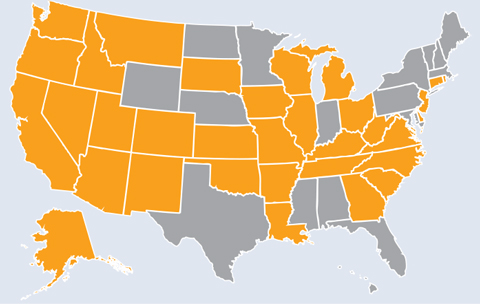 | Pain Med PrivilegesA number of states have reworded their drug laws following narcotic scheduling changes, allowing ODs to continue to prescribe narcotics and acetaminophen/narcotic combination drugs; other state’s laws were already strong enough to withstand challenges. Both are shown at left, depicted in orange. |
Fixing the Legislation
Several years ago, the FDA moved hydrocodone from schedule III to schedule II. “This change meant that ODs in many states would no longer be able to prescribe common narcotic analgesics,” such as an acetaminophen/hydrocodone combination, says Dr. Casella. He explains that there is a push for states to pass so-called “hydrocodone fix” legislation, adding this narcotic back to an ODs prescribing regimen. “We’ve accomplished this in Georgia, and a number of states have also passed such provisions in recent years.”
Incredibly, privileges can be jeopardized by something as simple as the language in legislation, inadvertently stripping the profession of rights its predecessors fought for and maintain through lobbying efforts.
“The DEA moved ODs to mid-level practitioner status years ago—who’s to say that if enough ODs let their DEA licenses lapse, we couldn’t continue to lose ground?” asks Dr. Casella. Use your privileges, he advises, because they allow you to care for patients in times of need.
“Hold your nose and pay the fee to renew,” says Dr. Ajamian. We’ve worked too hard not to.
