Editor’s Note: As part of our “Year in Review” retrospective, we’ve selected the top 30 news stories of the year and are re-sharing them as we close out 2022. Follow along as we count down to number 1!
This story was originally published on January 12, 2022.
No. 28 biggest news story of 2022:
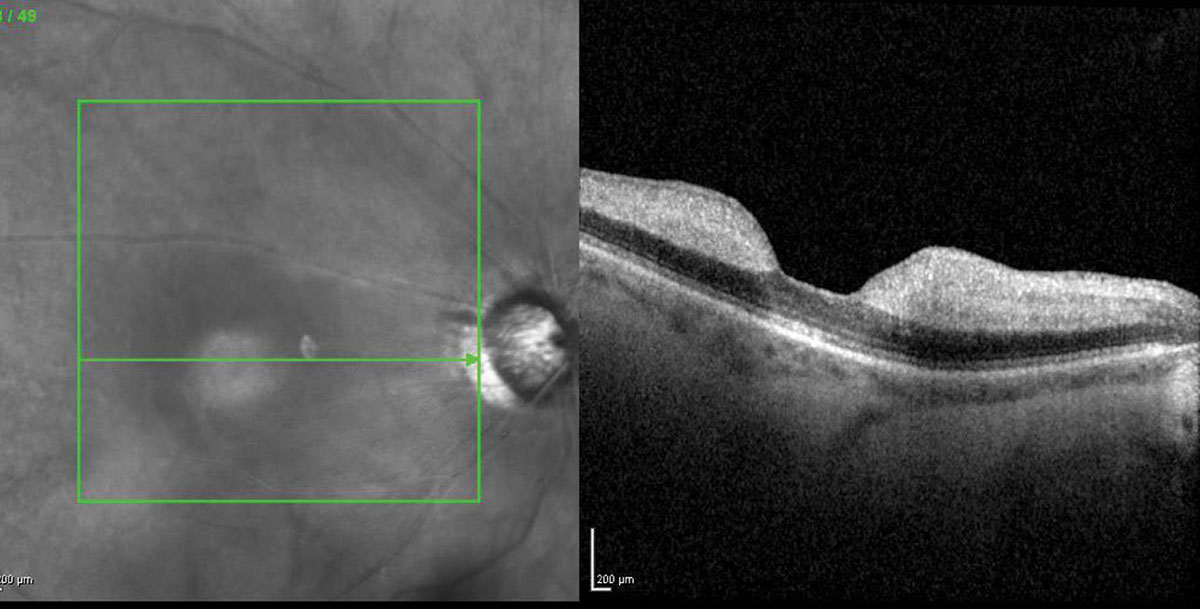 |
Patients with RAO are at increased risk of stroke and must be more urgently referred to stroke centers (pictured: CRAO). Photo: Jay M. Haynie, OD. Click image to enlarge. |
The American Academy of Ophthalmology (AAO) recently revised its Preferred Practice Pattern guidelines relating to retinal artery occlusions (RAO) to reflect those of the American Heart Association and American Academy of Neurology. This change comes on the heels of multiple studies that indicated acute RAO puts patients at a substantially elevated risk for stroke. The revised guidelines recommend urgent referral to a stroke center for any RAO.
“Historically, ophthalmologists have favored outpatient workup after RAO, as confirmed by surveys in 2009 and 2013 finding that <35% of ophthalmologists would refer a patient with RAO to the emergency room compared with >70% of neurologists,” wrote University of Pennsylvania Perelman School of Medicine researchers. They conducted a cohort study to determine how real-world practice patterns for referral and workup of incident RAO compare to the revised AAO guidelines and found that while they’ve improved, they’re still below the AAO’s new standard.
The cohort study included patients who received a new diagnosis of RAO (either central [CRAO] or branch [BRAO]) between 2002 and 2020, as identified in a large US medical claims database. The researchers reviewed the claims for AAO-specified diagnostic tests deemed “essential components” of RAO workup. These include carotid ultrasound, echocardiogram, magnetic resonance imaging (MRI) and emergency department (ED) referral.
They identified 18,697 new outpatient RAO diagnoses (11,348 BRAO and 7,349 CRAO). The percentage of patients who received diagnostic tests within seven and 30 days can be seen in Table 1. Only 4.1% of patients were referred to the ED within one day of diagnosis.
More ophthalmologists diagnosed RAO than neurologists (78.7% vs. 0.6%). The study authors noted that patients diagnosed by ophthalmologists were more likely to have a carotid ultrasound within seven days, but those diagnosed by neurologists were more likely to have an echocardiogram, MRI and ED referral. They reported that the rates of AAO guideline adherence increased significantly during the study period.
“Our analysis found that the rate of prompt referral for several of the key stroke risk screening tests recommended by the AAO for acute CRAO and BRAO is low, even if the time frame is extended out to one month after the diagnosis,” the investigators wrote. “This finding is in agreement with previous survey data for ophthalmologists, but substantially below what has been reported for neurology.” They noted that the rate of adherence to the AAO recommendations reached its peak in 2019, with a “presumably COVID-related reduction in referrals” in the first half of 2020.
“One of the surprising findings in this study is that although the rate of ED referral increased over time, the relative rate of referral was still small, particularly in light of the AAO guidance recommendations, first released in 2017 and then updated in 2020,” they continued. “Similarly, it was surprising that the rate of ED referral, carotid ultrasound, echocardiogram and MRI for patients were all significantly higher for CRAO compared with BRAO. While the odds of stroke are slightly increased with CRAO compared with BRAO, both [have been shown to] confer a considerable risk for future stroke, and the reduced referral rate may be related to a misconception that BRAO is a less medically significant diagnosis than CRAO. Also, BRAOs are more likely than CRAOs to present asymptomatically, which may cause the diagnosing physician to be less concerned over an imminent stroke, but again, the data and AAO guidelines do not support this line of thinking.”
“The multivariate analysis also revealed the unexpected finding of significantly more carotid ultrasound and echocardiogram testing for white and male patients compared with other races and female patients,” the authors noted. “The reasons for these findings are unclear but may point to another instance where health disparities exist between groups with similar future risks.”
They pointed out in their paper that their results must be interpreted within their data limitations. “First, for patients here, when RAO is first coded reflects the first diagnosis, but it doesn’t imply that the RAO has just occurred,” they wrote. “Ophthalmologists and clinicians report less urgent workup for RAOs that symptomatically have occurred more than one week previous. It’s still surprising, however, to see the overall low rate of these tests by 30 days. The code also doesn’t exclude an RAO associated with known or suspected giant cell arteritis, which if confirmed would obviate the need for certain tests here. If this was a significant contribution to the dataset, however, the rate of ED referral should be correspondingly higher.”
The authors concluded that full workup is more prevalent now, but that “the most recent rates suggest there is still work to be done.”
Table 1. Percentage of Patients Receiving Recommended Diagnostic Tests for RAO 2002-2020
Diagnostic Test | Received within 7 days (%) | Received within 30 days (%) |
Carotid ultrasound | 15.9 | 30.4 |
Echocardiogram | 9.4 | 21.1 |
Brain MRI | 4.9 | 8.1 |
Meer E, Scoles D, Hua P, et al. Recent practice patterns in acute retinal artery occlusions in the United States. Ophthalmic Epidemiology. January 4, 2022. [Epub ahead of print]. |
