 |
Adenoviruses have a variety of clinical effects on the body. Though most frequently associated with respiratory infections, they can also cause gastroenteritis, cystitis and rash illness—not to mention red eye.
Virology of Adenoviridae
Adenoviruses are non-enveloped, icosahedral shaped and contain a double-stranded DNA genome.They are categorized into four genera: Aviadenovirus (infects birds), Mastadenovirus (infects mammals), Atadenovirus and Siadenovirus (infect a variety of organisms).1,2
The virus enters the host by directly penetrating the cytoplasm or being engulfed into the cytoplasm through a membrane-bound vesicle, a process called endocytosis.
Transcription occurs in immediate-early, early and late stages. The virus sheds its DNA into the host nucleus, resulting in infection and the induction of the innate and cell mediated immune responses.3
 | |
| Adenovirus is so insidious that it’s being used as a viral vector in gene therapy. |
Clinical presentation varies and depends on both the serotype and the degree to which the infected host is immunocompromised.
Populations at Risk
Adenovirus infections are prevalent worldwide and are a significant cause of febrile respiratory illness in young children.2 Epidemics occur frequently in areas with infants or young children. Transmission occurs through different modes such as aerosol droplets, fecal-oral and contact with ocular secretions. Cervical secretions at birth can also transmit the virus from mother to neonate. Evidence that adenoviruses can be transmitted through organ transplantation suggests organs may harbor a latent form of the virus.1,2 Adenovirus can survive for long periods on environmental surfaces, contributing to its highly contagious nature.1,2,4
Treatment
Adenoviral systemic infection management generally consists of supportive therapy, as they are self-limiting conditions in healthy hosts. Treatment should only be considered in immunocompromised individuals. Using antiviral medications can pose a risk because of the associated drug toxicities. When treatment is warranted, ribavirin and Vistide (cidofovir, Gilead Sciences) therapies have variable success in immunosuppressed hosts.2
Adenoviral Eye Disease
Ocular manifestations of adenovirus are quite common and account for 65% to 90% of reported viral conjunctivitis cases worldwide.5 Symptoms of redness and irritation usually begin and predominate in one eye and may spread to the fellow eye within a few days. Patients frequently report a burning or foreign body sensation, and examination findings may include a watery, mucoid discharge. The lids may become red and edematous, and morning crusting is common. Preauricular lymphadenopathy is also commonly present.
Common Adenoviral Conditions in Humans
|
A history of antecedent upper respiratory tract infection or close contact with someone with a “red eye” is common. The severity of infection is variable in clinical presentation and may consist of follicular conjunctivitis (especially on the inferior palpebral conjunctiva), keratoconjunctivitis and (rarely) acute hemorrhagic conjunctivitis. Occasionally, pinpoint subconjunctival hemorrhages may develop.
The incubation period ranges from four to 10 days before the infection is clinically observable, which is due to the amount of time it takes for the virus to shed.5
Medical treatment of mild adenoviral conjunctivitis is not warranted, as it typically resolves within days to two weeks.5,6 Management is supportive, with cool compresses and artificial tears several times a day for comfort.
Epidemic Keratoconjunctivitis
Epidemic keratoconjunctivitis (EKC) is the term used when these highly contagious adenoviral eye infections further involve the cornea. EKC has the potential to impact long-term visual function.
Aside from the symptoms and signs consistent with a milder viral conjunctivitis, EKC may also present with more pronounced subconjunctival hemorrhages, moderate to severe lid edema and membrane or pseudomembrane formation. These membranes occur as a result of the inflammatory response and consist of leukocytes, fibrin and fibroblasts.
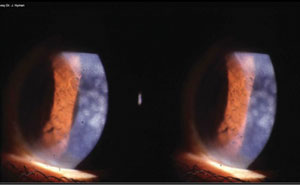 | |
| Subepithelial infiltrates from a viral conjunctivitis. Photo: Jeffrey Nyman, OD. |
The course of corneal involvement in EKC begins with punctate epitheliopathy within the first week, progressing to subepithelial infiltrates (SEIs) by week two. This accounts for symptoms of irritation and pain. It’s also the reason for decreased visual acuity, with SEIs that may last months to years after the infection subsides.5,7
EKC Detection and Treatment
Confirming adenovirus on the ocular surface is possible through rapid assay (AdenoPlus, RPS), cell culture combined with confirmatory immunofluorescence (CCIFA) or polymerase chain reaction (PCR). The latter two tests are not readily accessed by most optometrists. However, AdenoPlus is an in-office test with high sensitivity and specificity for adenovirus detection through a conjunctival swab sample. Results are available in 10 minutes, aiding in timely diagnosis.8
EKC is usually self-limiting, and treatment is reserved for cases of severe signs and symptoms, and for those who need the clearance of dense SEIs. Zirgan (ganciclovir gel 0.15%, Bausch + Lomb) showed significant inhibitory activity against some human adenoviruses (HAdV) that include EKC, suggesting it could be a candidate for the treatment of HAdV keratoconjunctivitis in the future. 9 Corticosteroids are effective in the elimination of SEIs, but have the potential for adverse effects (such as IOP rise) with long-term therapy.10 Researchers have demonstrated success using Restasis (cyclosporine A 0.05%, Allergan) in the clearance of SEIs with one month of use on average.11 Cyclosporine did not result in any ocular or systemic effects.
 | |
| Large pseudomembrane in an eye with EKC. | |
 | |
| Adenoviral conjunctivitis typically presents with inferior palpebral follicles. |
Due to the infectious nature of the virus and ease of transmission, you may implement Betadine 5% Sterile Ophthalmic Prep Solution (povidone-iodine, Alcon) to hasten resolution and reduce the likelihood of spread.12 Pseudomembranes should be manually peeled every two to three days. Topical corticosteroids may help prevent scarring.
Educate patients on the precautions they should take to prevent contagious spread, such as washing sheets and pillowcases, washing hands and taking a temporary leave of absence for those who work with the public and have active infection. In your office, thoroughly clean instruments and surfaces.
Good News About Adenovirus
While adenoviruses are associated with systemic and ocular infection, they may, in time, serve a beneficial role. They have the ability to affect several cell types to incorporate manufactured DNA into the host and have shown immense potential to function as gene vectors for vaccination and to treat a host of genetic diseases and cancers.13 Early clinical trials have demonstrated the use of this technique for the treatment of retinal disease, specifically in age-related macular degeneration and retinoblastoma.14
Adenoviral ocular infection is frequently encountered in the primary eye care practice. Proper detection and timely diagnosis of severe follicular conjunctivitis and EKC is essential in both treatment and prevention of transmission, as failure to do so can result in outbreak.
Dr. Labib is a resident at the Eye Institute, Salus University, Philadelphia.
1. Zhou X, Robinson CM, Rajaiya J, et al. Analysis of human adenovirus type 19 associated with epidemic keratoconjunctivitis and its reclassification as adenovirus type 64. Invest Ophthalmol Vis Sci. 2012 May;53(6):2804-11.2. Flomenberg P, Kojaoghlanian, T. Epidemiology and clinical manifestations of adenovirus infections. UpToDate. 2015:1-8.
3. Muruve DA. The innate immune response to adenovirus vectors. Hum Gene Ther. 2004 Dec;15(12):1157-66.
4. Russell W. Adenovirus: update on structure and function. J Gen Virol. 2009 Jan;90(1):1-20.
5. Yanoff M, Duker J, Augsburger J. Adenovirus. In: Ophthalmology 4th ed. St. Louis, MO: Mosby, 2004.
6. Bialasiewicz A. Adenoviral keratoconjunctivitis. Sultan Qaboos Med J. 2007 April;7(4):15-21.
7. Kanski, JJ. Clinical Ophthalmology. London: Butterworths; 1984. Print.
8. Sambursky R, Trattler W, Tauber S, et al. Sensitivity and specificity of the AdenoPlus test for diagnosing adenoviral conjunctivitis. JAMA Ophthalmol. 2013;131(1):17-21.
9. Huang J, Kadonosono K, Uchio E. Antiadennoviral effects of ganciclovir in types inducing keratoconjunctivitis by quantitative polymerase chain reaction methods. Clin Ophthalmol. 2014;8:315-2-.
10. Pihos A. Epidemic keratoconjunctivitis: a review of current concepts in management. Illinois college of optometry. 2012;1(9):69-74.
11. Okumus S, Coskun E, Tatar MG, et al. Cyclosporine a 0.05% eye drops for the treatment of subepithelial infiltrates after epidemickeratoconjunctivitis. BMC Ophthalmol. 2012 Aug;12:42.
12. Monnerat N, Bossart W, Thiel MA. Povidone-iodine for treatment of adenoviral conjunctivitis: an in vitro study. Klin Monbl Augenheilkd. 2006 May;223(5):349-52.
13. Flomenberg P, Kojaoghlanian T. Adenovirus and vector applications. UpToDate. 2015;1-7.
14. Sweigard JH, Cashman SM, Kumar-Singh R. Adenovirus vectors targeting distinct cell types in the retina. Invest Ophthalmol Vis Sci. 2010 Apr;51(4):2219-28.
EKC’s Pediatric Cousin PCF is seen predominantly in children and institutionalized individuals, with epidemics occurring within families, schools, prisons, ships and military organizations. Upper respiratory tract symptoms may precede ocular findings or may be absent. Acute conjunctivitis may occur with or without pharyngitis or a respiratory syndrome. Conjunctivitis usually begins in one eye and then spreads to the other, although both eyes may be affected simultaneously. Severe pain is atypical, but mild pain or discomfort, tearing, pruritus and morning crusting are common. Because PCF usually is a self-limited disease, ocular treatment is mainly supportive similar to that of mild to moderate adenoviral conjunctivitis. Corneal infiltrates are rare. Treatment with topical anti-inflammatory agents is reserved for cases with severe signs and symptoms. |
