History
A 45-year-old black female presented for a routine eye examination. She complained of mild nonspecific visual disturbance in both eyes at distance and near, which began eight months ago.
Her systemic history was significant for diabetes mellitus, for which she was medicated with Glucotrol (glipizide, Pfizer). She had no remarkable ocular history and denied ocular injuries or surgeries. She reported no known allergies.
Diagnostic Data
Her best-corrected entering visual acuity was 20/20 O.U. at distance and near. External examination was unremarkable. Her pupils were equal and reactive to light with no afferent pupillary defect.
The anterior segment examination was unremarkable. Confrontation visual fields were normal using the facial Amsler grid. Intraocular pressure by applanation tonometry measured 18mm Hg O.U.
The pertinent fundus findings are demonstrated in the photographs.
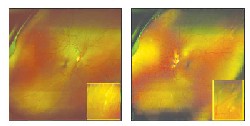 |
| A 45-year-old black female presented with this retinal appearance. |
Your Diagnosis
How would you approach this case? Does this patient require additional tests? What is your diagnosis? How would you manage this case? What is the likely prognosis?
Discussion
The diagnosis in this case is inactive multifocal chorioretinopathy of unknown etiology.
Additional testing included a frequency doubling automated visual field, color vision testing with Ishihara plates, photostress testing, brightness comparison testing and photodocumentation.
Multifocal chorioretinopathy is a diagnosis of exclusion.1-4 Other infectious and inflammatory retinopathies-such as sarcoidosis, tuberculosis, syphilis and other "white dot" syndromes-must be eliminated before a positive diagnosis can be made.4
Additional systemic testing may include:1-4
Full blood work-up to rule out inflammatory or infectious etiologies.
Angiography to rule out multiple evanescent white dot syndrome (MEWDS), acute multifocal posterior placoid epitheliopathy (AMPPE) and choroidal neovascularization (CNV).
Threshold visual field testing to quantify any defects.
Three-mirror macular evaluation to rule out cystoid macular edema and birdshot chorioretinitis.
Multifocal chorioretinitis is an idiopathic chorioretinal inflammatory disease that typically presents in an otherwise healthy individual. It has a predisposition for women in the third decade and is bilateral 75% of the time.2
The typical clinical retinal appearance involves multiple, bilateral, discrete yellow or white circumscribed lesions that can appear intraretinal, but by definition usually involve the retinal pigment epithelium, Bruch"s membrane and the choroid. If the lesions appear in the posterior pole, the patient can present with decreased visual acuity.4 An anterior chamber inflammation is common, and can be present in up to 50% of cases.1,2 The condition is typically chronic and recurrent, which dictates periodic monitoring for signs of active inflammation (presenting as a mild vitritis or a mild uveitis).4
1. Dreyer RF, Gass DJ. Multifocal choroiditis and panuveitis. A syndrome that mimics ocular histoplasmosis. Arch Ophthalmol Dec 1984;102(12):1776-84.
2. Gass JD. Multifocal choroiditis and panuveitis. In: Gass JD. Stereoscopic Atlas of Macular Diseases: Diagnosis and Treatment, 4th ed., vol. 2. Philadelphia: Mosby, 1997:688-90.
3. Lardenoye CW. Peripheral multifocal chorioretinitis: a distinct clinical entity? Ophthalmology Nov 1997;104(11):1820-26.
4. Shuler MF, Regillo CD. Multifocal choroiditis. In: Rapuano CJ. Retina: Color Atlas & Synopsis of Clinical Ophthalmology. Philadelphia: McGraw-Hill, 2003:127-129.
