|
|
 |
Clinicians are well aware of the hallmark symptoms of dry eye, but if you based your decision to treat solely on symptoms, you might be missing some diagnoses; research shows that fewer than 60% of patients with dry eye disease (DED) are symptomatic.1 Often overlooked, but equally critical, is an awareness of predisposing factors that raise a patient’s risk level. Connecting these two is one of the most important steps in developing a successful ocular surface disease protocol.
This article will consider how predisposing factors combined with key findings become paramount to making a proper diagnosis and eventual treatment.
When Signs and Symptoms Don’t Correlate
In most conditions we encounter as optometrists, symptoms are paramount. For example, we judge our management of allergic conjunctivitis to be a success when a patient responds to treatment with an absence of itching, redness and swelling. Adopting this strategy—basing success on the relief of symptoms—works well for most ocular disease states and results in happy patients and a successful clinical outcome. But in DED, many patients with symptoms of dryness, grittiness, burning or stinging may not actually have “dry eyes,” and thus a treatment that targets dry eye would likely not alleviate symptoms.2
The result would be a patient returning with the same symptoms, and often more frustrated than before. They may even seek out another doctor.
For example, a patient experiencing dryness, fluctuating vision and gritty, burning eyes (especially late in the day or while using a computer) may actually have convergence insufficiency, vertical disparity computer vision syndrome or other eye alignment issues.3 This patient would receive a much better response from visual training or prism in their spectacles, or both, than any dry eye therapy. Other non-DED causes of similar symptoms include anterior blepharitis etiologies (e.g., Demodex), contact lens solution issues (e.g., corneal infiltrates), allergic conjunctivitis, epithelial membrane dystrophy/mild recurrent corneal erosion, pingueculitis, giant papillary conjunctivitis, Salzmann’s nodular degeneration, conjunctivochalasis and others.4-8
|
|
|
|
|
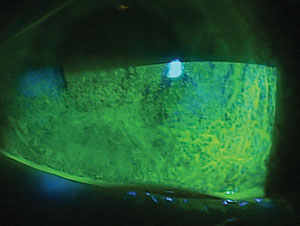
Advanced neurotrophic keratitis, a condition that can decrease corneal sensitivity—and thus reduce symptomatic complaints. That could lead to a missed diagnosis.
|
In some circumstances, a patient with one of these conditions may experience mild resolution of symptoms when treated with classic dry eye therapies, but in many cases it will never fully resolve with an approach that targets DED.
At the other extreme, some of the worst cases of DED actually present with little to no symptoms. A patient suffering from severe dry eye who is largely asymptomatic (other than perhaps blurred vision from the advanced ocular surface disease findings) likely has a neurotrophic cornea.9 These include patients with active Sjögren’s syndrome, diabetes and those in the immediate aftermath of a herpes simplex keratitis, herpes zoster outbreak, a course of chemotherapy or radiation treatment. New research into neurotrophic keratitis shows a decreased corneal sensitivity secondary to decreased sub-basal corneal nerve length.10 This decreased sensitivity results in loss of sensation and a decreased blink rate, which only further exacerbates the condition.11
These patients are most in need of care; if symptoms were your sole determinant, they would be missed. Unfortunately, many such patients are overlooked, frustrated and seeking doctors who understand ocular surface disease management. A recent Harris Interactive study showed that only 29% of patients with true DED felt their optometrist provided adequate care and knowledge of their disease.
Suspicious Minds
It is a foundational principle of medical care that a proper diagnosis is the most important step to treatment. But if symptoms are not reliable, how might we make the proper diagnosis?
|
Blur: Consistently Present, Consistently Misconstrued
Perhaps the only key symptom reported with almost all levels of dry eye disease is blurred vision, whether it’s transient blurred vision secondary to tear film instability in early disease or persistent blurred vision secondary to central corneal staining in advanced disease. The problem: most clinicians don’t consider dry eye as the primary diagnosis when they encounter a complaint of blurred vision. If the patient can be corrected to 20/20, that is often assumed to be the solution and the patient receives a non-medical diagnosis; in actuality, dry eye is perhaps the most common cause of blurred vision—and is truly a medical condition. |
|
One way to raise your probability of success is to employ advanced testing such as osmolarity, meibo-graphy, true dry eye staining, meibomian gland expression, blink analysis and other precise measures now clinically available.12 But as many doctors just starting out may not have access to these technologies, another important determinant is to look at the number of predisposing factors a patient may display.
This approach alone may not be 100% accurate in establishing a diagnosis, but combined with testing, it can help confirm the disease.
A patient with a significant number of these predisposing factors may heighten the clinician’s suspicion of DED. When the level of suspicion is commensurate with risk factors, implementing and understanding dry eye diagnostics can point to the cause and true diagnosis.
Advanced Testing Options
As an example, I recall using osmolarity testing when it was first approved and had a series of patients with consistently normal osmolarity measurements. I’d look at the patient and ask them about their symptoms; they described their eyes as dry, gritty and burning with fluctuating vision that worsened late in the day and especially while reading or spending significant time on a computer. An expert in the field of binocular vision and eye alignment enlightened me and visited my clinic to help. He discovered that nine out of 10 patients that day had eye alignment issues, and he was able to resolve all of their symptoms with appropriate binocular vision management. I had a whole new respect for the accuracy of these advanced testing options and a newfound humility about what I thought was my advanced clinical knowledge in the field.
|
|
Key Predisposing Factors
|
Since then, I’ve gleaned many other insights that have changed how we run our ocular surface disease clinic to achieve highly successful outcomes in some of the most advanced OSD referrals.
Dry eye is a complex condition to manage. But the critical first step is identification—with as much specificity as possible. Understanding the predisposing factors, realizing that signs and symptoms may not align and learning about new diagnostic technologies will aid clinicians in making the right diagnosis.
From there, an appropriate treatment becomes much more likely, resulting in successfully managed OSD patients.
1. Bron AJ, Tomlinson A, Foulks GN. Rethinking dry eye disease: a perspective on clinical implications. Ocul Surf. 2014 Apr;12(2 Suppl):S1-31.2. Sullivan BD, Crews LA, Messmer EM. Correlations between commonly used objective signs and symptoms for the diagnosis of dry eye disease: clinical implications. Acta Ophthalmol. 2014 Mar;92(2):161-6.
3. Jatinder B, Naveen N, Renu TB. Computer vision syndrome: A review. Journal of Clinical Ophthalmol. 2014;2(1):61-8
4. Guillon M, Maissa C, Wong S. Symptomatic relief associated with eyelid hygiene in anterior blepharitis and MGD. Eye Contact Lens. 2012 Sep;38(5):306-12.
5. Sankaridurg PR, Sweeney DF, Holden BA, et al. Comparison of adverse events with daily disposable hydrogels and spectacle wear: results from a 12-month prospective clinical trial. Ophthalmology. 2003 Dec;110(12):2327-34.
6. Hom MM, Nguyen AL, Bielory L. Allergic conjunctivitis and dry eye syndrome. Ann Allergy Asthma Immunol. 2012 Mar;108(3):163-6
7. Asbell PA, Torres MA. Therapeutic dilemmas in external ocular diseases. Drugs. 1991 Oct;42(4):606-15.
8. Balci O. Clinical characteristics of patients with conjunctivochalasis. Clin Ophthalmol. 2014 Aug;8:1655-60
9. Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clin Ophthalmol. 2014 Mar;8:571-9.
10. Lambiase A, Sacchetti M, Mastropasqua A, et al. Corneal changes in neurosurgically induced neurotrophic keratitis. JAMA Ophthalmol. 2013 Dec;131(12):1547-53.
11. Gillan WDH. Repeatability and reproducibility of Tearlab. S Afr Optom. 2013;72(1):19-24.
12. Shaheen BS, Bakir M, Jain S. Corneal nerves in health and disease. Surv Ophthalmol. 2014 May-Jun;59(3):263-85.
13. Dry Eye Workshop. The Ocular Surface Journal. April 2007 5(2).
