 |
A 53-year-old woman presented urgently with a moderately painful red right eye of two days duration. She reported some associated tearing but no other discharge. She denied itching or recent illnesses. It seemed to be neither better nor worse than when she first noticed the pain, which she had awoken with. This was a first occurrence for her. Her medical history was significant only for unspecified thyroid dysfunction.
Her corrected visual acuity was 20/20 in each eye. She manifested a sectorial redness in her right eye, and the remainder of her external evaluation was normal. Her intraocular pressure was 22mm Hg OU. A dilated fundus exam revealed optic disc cupping of 0.3/0.3 in each eye and normal retinal findings OU. Following dilation, in which 2.5% phenylephrine was employed as part of the regiment, her redness has significantly reduced but did not completely dissipate. Based upon her symptoms and clinical examination, she was diagnosed with episcleritis.
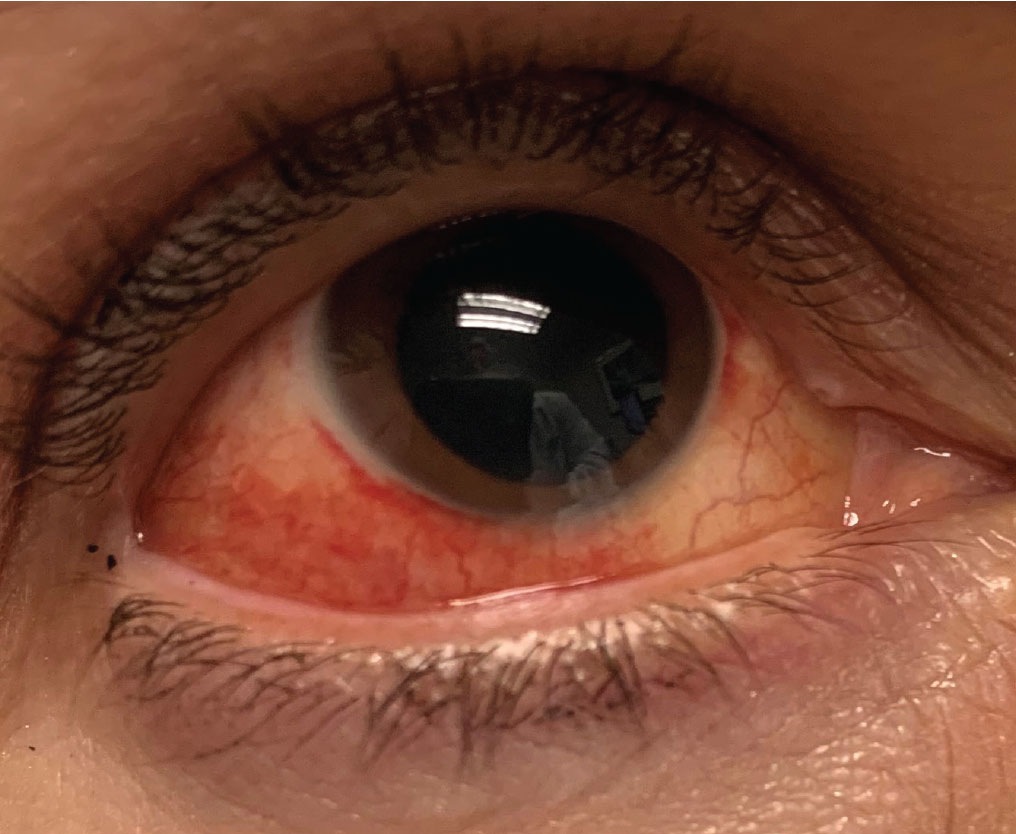 |
| Sectoral injection in episcleritis. Click image to enlarge. |
In the Red
Episcleritis is a superficial inflammation involving the conjunctiva and episcleral region.1,2 The episclera is a highly vascularized ocular tunic that encircles the globe between the overlying conjunctiva and the underlying sclera.3,4 The inflammatory response remains localized to the superficial episcleral vascular network with nongranulomatous inflammation and vascular dilatation with perivascular infiltration.3-5 Episcleritis commonly appears as a sectorial injection involving both the episcleral tissues and overlying conjunctiva, usually concentrated in either the nasal or temporal quadrant.
Typically, there is no discharge but tearing may be common.1,2 Any significant discharge should prompt consideration of other possible entities rather than episcleritis. Significant serous discharge may indicate a viral conjunctivitis, but the eye is usually diffusely rather than sectorally red. Mucopurulent discharge and eyes that are stuck shut upon awakening points to a bacterial infection. Tearing and significant itching prompt thoughts of allergic conjunctivitis and patient rubbing may induce sectorial injection. True episcleritis occurs in response to noxious stimuli or secondary to an underlying systemic disease.3,4 Quite commonly, episcleritis reveals no underlying etiology and remains idiopathic.
Episcleritis typically appears acutely with patients often reporting that they woke up with a red eye. Superior injection has the potential to go unnoticed and may be completely masked by the upper eye lid. Most cases are unilateral; however, it may occur bilaterally in cases of toxic exposure or underlying systemic disease.
There may be a translucent white nodule within the inflamed area. When this finding is present, it is called nodular episcleritis. Nodular episcleritis represents a focal concentration of inflammation. The nodule adheres to underlying tissue and is distinguished from conjunctival cysts and phlyctenules by its subsequent lack of mobility with the conjunctiva. Patients may complain of mild pain or tenderness to the affected region, pain upon manipulation or a stabbing sensation upon moving the eyes. Due to lack of corneal involvement, visual acuity is unaffected. Though the cornea is inherently unaffected, long-standing or recurrent episcleritis may precipitate dellen formation. Though uncommon, it is possible anterior chamber cells may be seen in more pronounced cases.
Care must be taken to distinguish episcleritis from the more severe condition scleritis, which may appear superficially similar. Ocular injection is typically deeper with scleritis and the eye will not blanch with 2.5% phenylephrine as it would in episcleritis. Pain is much more common and severe in scleritis compared to episcleritis. Some patients with scleritis complain of a boring type of pain which does not occur in episcleritis. Additionally, vision is more likely to be reduced in scleritis due to more widespread inflammation whereas there should be no significant vision loss in episcleritis unless there is a mild concurrent keratopathy.
Not every case of sectorial injection is true episcleritis. Trichiasis or other observable irritation, may mechanically induce a “pseudo-episcleritis.” Careful history and examination should identify potential mechanical causes of sectorial injection that may be mistaken for true episcleritis. Treating these entities without first removing the cause may result in management failure or, at least, unnecessary prolonged treatment. Signs and symptoms should be considered before prescribing any medications.
 |
| Episcleritis can present with complaints of discomfort or irritation (rather than true eye pain), redness and edema to the affected area over the sclera. Click image to enlarge. |
Treatment
Most cases of episcleritis will blanch with the application of topical 2.5% phenylephrine, which aids in diagnosis.3 In contrast, deeper ocular inflammation such as seen in scleritis and uveitis will not result in blanching, and pharmacologic use does not affect the clinical appearance.
Episcleritis may be idiopathic or in association with some underlying systemic disease. Among those conditions associated with chronic or recurrent episcleritis include rheumatoid arthritis, polyarteritis nodosa, systemic lupus erythematosus, inflammatory bowel disease, sarcoidosis, Wegener’s granulomatosis, tuberculosis, Lyme disease, gout, herpes zoster and syphilis.6-9 Inflammatory bowel disease is a strong consideration when encountering patients with episcleritis.10
Most cases of episcleritis are self-limiting, resolving spontaneously within two to three weeks even in the absence of treatment.11 Patients who are symptomatic or disturbed by cosmetic appearance benefit from a regimen of cold compresses, lubricants, topical nonsteroidal anti-inflammatory drugs and topical corticosteroids.11 As inflammation in episcleritis is relatively superficial, virtually all topical steroids are acceptable, including fluorometholone, rimexolone, loteprednol, prednisolone and difluprednate. Dosing on both the topical NSAID and topical steroid typically range from BID to Q4H. Cycloplegia is rarely necessary.
Recalcitrant or severe cases associated with systemic disease may require oral therapy which could include ibuprofen (600mg to 800mg BID to QID), naproxen sodium (250mg to 500mg TID) or indomethacin (25mg to 75mg BID).1,11 Follow-up on these cases should be weekly until resolution or marked improvement. Patients placed on steroids of any kind are at risk for steroid-induced elevation of intraocular pressure, which should be monitored and addressed with glaucoma medications if necessary. Prolonged cases of episcleritis are atypical and should prompt consideration of other diagnoses or increased likelihood of an underlying systemic association.
Due to the association with systemic disorders, patients with exaggerated, recalcitrant or recurrent events should be referred for a medical evaluation with either an internist or rheumatologist. Recommendations should be made for a complete autoimmune profile and assessment of the aforementioned systemic associations with emphasis on inflammatory bowel disease.
The patient presented here was educated about her condition and prescribed topical prednisolone acetate 1% QID. She missed her scheduled follow-up appointment but telephoned a week later to say that her discomfort and redness resolved. She was instructed to initiate a brief steroid taper.
Takeaways
Although there are many things to keep in mind when encountering episcleritis, it is a condition similar to subconjunctival hemorrhage in that it typically looks worse than it is and is self-limiting in most cases.
Dr. Sowka is an attending optometric physician at Center for Sight in Sarasota, FL, where he focuses on glaucoma management and neuro-ophthalmic disease. He is a consultant and advisory board member for Carl Zeiss Meditec and Bausch Health.
1.Kirkwood BJ, Kirkwood RA. Episcleritis and scleritis. Insight. 2010;35(4):5-8. |
