Doctors, technicians and opticians all play a critical role in the potential success of a child’s visual performance—and some kids require a little more creative thinking by every care provider on the team. These unique spectacle wear challenges help to illustrate the many methods you can employ—including new frame technology, innovative lens design and motivating techniques—to ensure your pediatric patient’s spectacle success.
Everyday Challenges with Real World Solutions
Most pediatric patients are prescribed spectacles and instructed to return for follow up to check their response to the glasses after two to three months of wear. In cases where visual acuity has not improved with spectacle wear and amblyopic factors continue to linger, one culprit is often to blame: patient compliance.
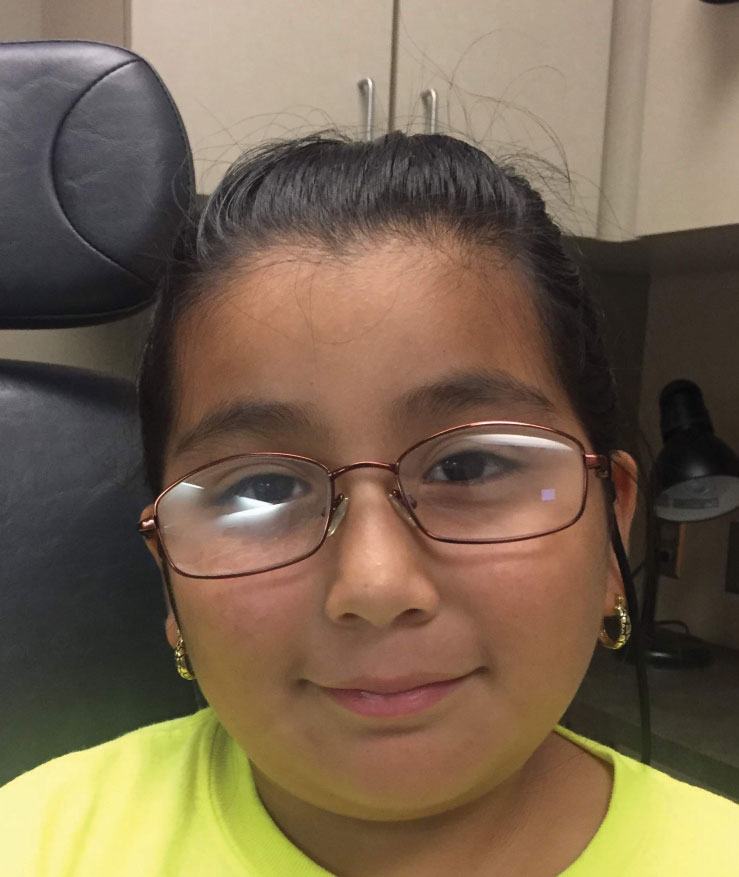 |
| Fig. 1. This child’s small pupillary distance and round head presents a fitting challenge. |
Non-compliance typically involves parents, peers, spectacle fit, prescription or some combination of all of these. It is important to anticipate these reasons during your exam and address them when spectacles are first prescribed to increase the likelihood of good spectacle wear habits from the beginning. If we don’t, the child could completely miss the opportunity for improved visual development and be stuck with poor vision in one or both eyes. These cases exhibit the top reasons for non-compliance in the pediatric spectacle-wearing population:
Pessimistic parent. A three-year-old black female was referred by her pediatrician for reduced acuity OD. She had anisometropic hyperopia OD>OS with reduced best-corrected acuity OD. She was a cooperative child, but as three-year-olds will do, she got antsy by the end of the exam. At this point, her mother said, “If you don’t sit still, they are going to give you glasses.” This negative take on glasses laid the groundwork for an uphill battle in compliance right out of the gate.
Solution: Your most formidable tool in combating a situation such as this is good communication with both the patient and parent. When you announce that glasses are the best vision correction option, it is important that the parent understands why glasses are prescribed, how they will help their child see better and what to anticipate when first trying the glasses. Reassure the parents that you only prescribe glasses when: (1) they are absolutely necessary and (2) they will improve the child’s quality of life.
The final prescription may take one or two additional visits every three months to monitor for stability or to verify that the objectively measured refractive error is measured consistently.
Once you have finalized the prescription, these tips can help you increase compliance and maximize vision potential:
• Make a trial frame of the “opposite prescription” for the parent. This allows them to see for themselves that vision may be functional, but far from perfect.
• Try a game of I-spy with new glasses, pointing out objects in the distance that, prior to correction, the child could not see.
• Explain the importance of wearing glasses: there can be no negotiating. Glasses should be worn at all times or risk permanent vision deprivation. Parents should understand that glasses wear can be as important as using a car seat.
• Give the child some of the responsibility. Some useful phrases include: “When they’re not on your face, put them in your case” and “There are only two times when you don’t have to wear your glasses. Can you guess? If you’re not in the tub and not in the bed, where should your glasses be? On your head.”
• Find the patient’s motivation. If the glasses help improve binocular vision and stereopsis, this might be just what the athlete and athlete’s parents want to hear. The fear of not passing a driver’s license vision test can be a significant motivation for older patients. Find out your state’s vision requirements for driving and try to get your amblyopes to that level at a young age. Otherwise, it may be difficult to develop good vision by the time they are old enough to drive.
Peer pressure. A five-year-old Hispanic female was referred by her pediatrician for reduced visual acuity OU. Her isoametropic high mixed astigmatism was fully corrected with glasses, which was prescribed for full-time wear. Upon returning for visual acuity check, her mother reported that the child loved her glasses the first day she got them! However, after a single day at school with her new style, the child refused to wear them.
Solution: There are phases in school-aged children when everyone seems to want glasses, and other times when no one wants glasses. The Children’s Attitudes about Kids in Eyeglasses study showed 24 paired photos to 80 kids (8.3 years +/- 1.3 years) and asked a series of questions about participants’ perception of the children in the photos.1 In response to, “Which child looks smarter?” children were more likely to choose the spectacle wearer. The participants showed no significantly different perceptions of kids wearing glasses for all other questions.
Nonetheless, kids are often driven by peer pressure, and negative attention due to glasses wear can thwart compliance quickly. Words of encouragement during the glasses fitting and dispense, citation of age-appropriate TV personalities, sports icons and even wearing fun glasses yourself during the exam can increase positivity about their new prescription and encourage wear.
Perfect prescription, imperfect fit. A seven-year-old Hispanic female was referred from a school screening for reduced visual acuity OU. She had anisometropic high hyperopia and high astigmatism OS>OD. The child was given a prescription that fully corrected the anisometropia and the astigmatism, but the hyperopic prescription was cut symmetrically by one diopter to maximize adaptation to high cyl glasses. At follow-up, her visual acuity had only slightly improved. While her mother stated that the child did try to wear her glasses, the glasses fit poorly and fell off of her nose. The patient’s face was slightly too wide for child frames, but her pupillary distance was too narrow for the adult frames (Figure 1).
Solution: During our exam, it is easy to think that getting the correct prescription may be the most meaningful aspect of our care. However, if we are unable to fit a pediatric patient in spectacles that are comfortable, stable and provide adequate optics, the prescription is fruitless. Children are unique and have many features that can challenge an ideal spectacle fit. For example, a flat bridge and round cheeks can keep glasses from staying in place, or a high level of physical activity can increase the risk that glasses are broken during wear.
When prescribing for the pediatric population, you or your optician should help them select frames based on stability, durability and protection. These pointers can help you master pediatric fitting:
• Consider spring hinges, frames that do not rest on cheeks and frames that do not put the entire weight of the frame on one location.
• For highly astigmatic glasses, choose round frames to avoid asymmetric edge thicknesses.
• For highly hyperopic glasses, avoid frames that sit close to the eyes to avoid lashes hitting the centers. Metal frames or frames with nose pads can help pull the frame out a bit for those with extra long eyelashes.
• For high myopes, avoid large or semi-rimless frames that increase edge thickness and lens weight.
• For all high prescriptions, vertex distance and pupillary distance should follow the carpenter’s rule: measure twice, cut once.
• Avoid choosing glasses with the assumption that the patient will grow into them. Kids will generally not grow enough in one year to warrant changing the frame.
• Avoid using adult frames on kids when the pupillary distance is small and the patient’s head is round or wider in the spectacle area. The patient’s eye should be centered horizontally to avoid decentration (Figure 2). Temples should not touch the sides of the head until right before the ear. If you can stick a pencil or your finger between the temple of the frame and the side of the patient’s face, it’s too big.
 |
| Fig. 2. Compared with the child in Figure 1, this patient was fit with glasses that placed the pupils in the center of the frame and with less wasted lens space temporally. |
Tricky Prescriptions
There are times when a child reports they can see just fine without glasses or can see no better with them—and they may be right. Anisometropic patients, those with high astigmatism and even high myopes often need glasses to help with more than simply clearer vision:
• Anisometropic patients who have one eye with minimal prescription and one eye with a significant prescription often have no visual complaints. However, covering the better-seeing eye helps to show the child what it would be like if he lost his better-seeing eye. Polycarbonate or Trivex lenses are required for these children for extra protection.
• Patients with significant astigmatism often see 20/30 with and without glasses. Here, patient and parent education is key once again. Explain that with continual wear, vision will get noticeably better with time and with the right prescription.
• Patients with highly hyperopic glasses may see worse in their glasses. Explain that the eyes are doing too much work without glasses, like carrying around five-pound dumbbells. The glasses will help the child see more comfortably, not just more clearly. If, after one to two follow ups with minimal to no glasses wear, consider prescribing one drop of atropine 1% in each eye on a Saturday and Sunday. Explain to the parent that this restricts the child’s ability to accommodate through their prescription, which helps them avoid working their eyes too hard. It also helps to demonstrate to the child that the glasses improve blurry vision. This may allow for adaptation to the feeling of the glasses, as well as the diffraction and peripheral changes that come with moderate to high hyperopic prescriptions.
Pediatric Prescribing ResourcesFor specifics on refractive error prescribing recommendations, visit www.aoa.org, following the prompts: Home > Optometrists > Tools & Resources > Clinical Care Publications > AOA Optometric Clinical Practice Guidelines. Another valuable resource for prescribing is www.pedig.jaeb.org. This public website of NIH-funded research shares results from many clinical trials involving amblyopia and other pediatric ocular conditions that will help guide prescribing decisions. |
Extra Bells and Whistles
The optometric oath indicates that we have committed to offering our patients the spectrum of available options for eye care. The average progression of myopia is about 0.50D per year in the school-age group, but that’s just an average.2 In addition, kids can easily lose or break their glasses. While many ODs consider these good reasons to offer basic packages for kids that include a sturdy, warrantied frame and polycarbonate, shatter-resistant lenses, some upgrades might serve the patient better:
• Anti-reflective coating. Reducing glare into and off of the lenses may make the difference between good compliance and no compliance. A thorough literature search can help you decide if this age group could benefit from AR coating that blocks blue light. Some blue and ultra-violet light is good when used to help the body manufacture vitamin D and when such high-energy visible light helps boost alertness. Light also influences the circadian rhythm. Some of the eye’s components have diurnal variations associated with high lights (like being outside) and low darkness (turning lights out before bed), which seems important in accurate eye growth. On the other hand, excessive use of devices that emit blue light may affect vision in a less positive way, such as when the eyes are strained from extended use. Blue light has also been shown to suppress melatonin, the hormone that promotes sleepiness, suggesting that blue-light emitting devices used before bed have the potential to impact the body’s circadian rhythm.3-5
• Trivex lenses. These are shatter resistant, thinner and lighter—all of which can improve the cosmesis of high prescriptions.
• Photo-sensitive or prescription sunglasses. These may seem like an extravagance, but the clear media of the eye in this age group may make childhood the most vulnerable age for sun exposure.
 |
| Fig. 3. As the neonate aphakic patient with micro-ophthalmia ages, the difference in eye size becomes more prominent. A magnifying plus lens may make the eyes appear more equal. |
Unique Challenges with Creative Solutions
Kids with special needs and facial features that make for a poor fit with conventional frames present an entirely different set of challenges. You have to get creative and search the best prescribing recommendations to find the life-changing result your patient needs. These cases help illustrate some of the necessary out-of-the-box solutions:
Unilateral trauma. A two-year-old African American female was referred for evaluation following trauma that included a fork to her right eye. This resulted in high anisometropic refractive error post lens extraction. Her left eye had a minimal refractive error, which allowed her good visual function. As such, the patient had been without correction since surgery four to five months prior. Examination determined that she had a refractive error of +15.00D OD.
Polycarbonate spectacles were prescribed for protection of the phakic eye as well as to correct refractive error. A cable temple and a sturdy bridge were chosen to distribute the weight of the high plus spectacles. Because of her recent high refractive anisometropia, the patient was instructed to patch her phakic left eye.
With many aphakic patients, our aim is the get them into extended wear contact lenses for best optical benefits. Even with aphakic contact lenses, it is important to maintain polycarbonate spectacle lens over-wear for protection.
Aphakia and micro-ophthalmia. A neonate African American female patient with a history of recent lens extraction and micro-ophthalmia OS presented for a contact lens fit (Figure 3). During her early years, contact lenses will be used to maximize the visual potential OS. But when she is old enough to care about the visible difference in size between her eyes, the power of the contact lens in the aphakic eye can be modified so that a hyperopic polycarbonate lens can be placed in front of the left eye. The result will be relative magnification of the smaller eye to balance the appearance of the size of the eyes.
No earpieces, no problem. A four-year-old Asian male presented with his mother for evaluation of an eye turn that required glasses. The patient, who had been adopted from China at 18 months of age, had no ears. Even when he eventually received ear prosthesis, they would be quite fragile. Without any commercial frames that do not require stabilization with earpieces, custom spectacles were made (Figure 4). The patient’s glasses had a plastic cable that vaulted over and behind his head.
Sensory sensitivity vs. spectacles. A six-year-old female with a sensory disorder presented for evaluation after having suffered a concussion. She had never worn spectacles before and was found to have a moderate hyperopic prescription. The patient was currently undergoing occupational therapy to work on wearing shoes, blue jeans, shirts with tags and jackets—all of which were uncomfortable for her. She could not stand to wear the prescribed glasses for more than a few minutes at a time, yet was still symptomatic while reading uncorrected.
We called the patient’s occupational therapist and worked together on a plan to increase spectacle wear time. At a follow up visit seven months later, the patient could now wear sandals, blue jeans and glasses for a few hours at a time—a huge step forward. Comanagement and communication with the patient and her mother during examination and at dispense turned the challenge of a sensory disorder into a spectacle wear success.
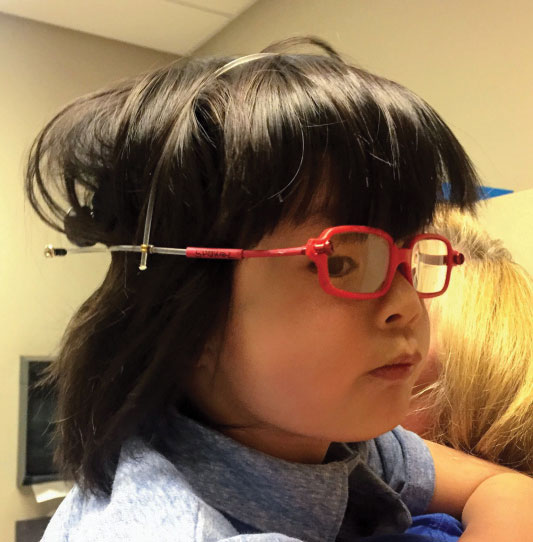 |
| Fig. 4. This four-year-old boy has long hair to hide the absence of ears. Thanks to specialty frames, the glasses fit perfectly on this active boy. |
Frame Technologies
Many newer technologies exist to improve spectacle wear in pediatrics patients, including bendable frames, Flexon metal (Marchon Eyewear), straps behind the head and silicon “keep-ons” to fit behind patients’ ears. However, these needs cannot be met without a clinician who is informed about options and knows how the patient can best access these technologies. If you do not serve a large pediatric population, it may not be profitable for you to keep many styles in your optical. Attend local society meetings to find out which opticals near you carry and can fit pediatric and specialty pediatric frames. The exhibition hall at conferences and trade shows can be a great place to browse a high volume of pediatric frames.
Children are not little adults—a truth in the exam room and optical space. If you take the time to get the right pediatric prescription, take the additional time and effort to prescribe the perfect fit. No one ever says, “Wow, that prescription looks great!” Understanding new frames technologies, being smart with lens design and discovering what motivates your patients will allow you to be successful beyond your exam room. Those glasses are not only your walking billboards, they are the springboards to your patients’ future successes.
Dr. Galt recently completed her residency in pediatric optometry at the University of Alabama at Birmingham (UAB) School of Optometry. She is currently working at a multidisciplinary pediatric private practice in Denver.
Dr. Weise is director of the Pediatric Optometry Service at UAB Eye Care. She served as the Correction of Myopia Evaluation Trial (COMET) investigator, studying nearsightedness in children through the NIH from 1997 to present. She is the co-protocol chair on another NIH-funded trial studying myopia and atropine, and is the team eye doctor for UAB Blazers football.
Ms. Baldwin is a licensed dispensing optician trained at Duke University. She also served as the NIH-funded COMET Optician at UAB for more than 10 years.
1. Walline JJ, Sinnott L, Johnson ED, et al. What do kids think about kids in eyeglasses? Ophthalmic Physiol Opt. 2008;28(3):218-24. 2. Gwiazda J, Hyman L, Hussein M, et al. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Ophthalmol Vis Sci. 2003 Apr;44(4):1492-500. 3. American Academy of Pediatrics. Council on Communications and Media. Media use in school-aged children and adolescents. American Academy of Pediatrics Policy Statement. 2016. http://pediatrics.aappublications.org/content/early/2016/10/19/peds.2016-2592. Accessed July 27, 2018. 4. Heiting G. Blue light: it’s both bad and good for you. All About Vision. www.allaboutvision.com/cvs/blue-light.htm. Accessed July 27, 2018. 5. Gringas P, Middleton B, Skene DJ, Revell, VL. Bigger, brighter, bluer-better? Current light-emitting devices – adverse sleep properties and preventative strategies. Front Public Health. October 13, 2015. www.frontiersin.org/articles/10.3389/fpubh.2015.00233/full. Accessed July 27, 2018. |
