I commend you for your choice of topics in the December 15, 2004, issue of Review of Optometry, particularly the article, Your Role in Fall Prevention. Although many issues can contribute to increased likelihood of falling in the elderly, one visual concern was omitted in this article. The automatic function of balance is one of the most significant issues for many elderly. They are not always able to do tasks that require balance without devoting conscious attention to not falling. Vision makes a significant contribution to balance.
 |
Balance is enhanced when all systems are in sync, such as when a person is walking and looking ahead at the horizon. However, people should also be able to maintain their balance independent of vision. For example, people may close their eyes when taking a shower. We maintain balance independent of vision even more frequently when we are walking and look to the side,
or even just stand and turn our heads. These skills tend to decline over time but are amenable to therapy.
As optometrists see more and more elderly patients, we can help them decrease their chances of falling. This will become a more important aspect of the care we provide and may be considered another aspect of primary eye and vision care.
Gary J. Williams, O.D.
Owego, N.Y.
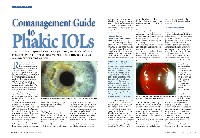
Advances in Changing Times
How times have changed! Regarding the article, Comanagement Guide to Phakic IOLs, its interesting to see that there is surgery for just about anything these days.
 |
In the old days when I was in practice, cataract removal would have given a high myope decent vision without an IOL. Of course, for moderately high myopes, perhaps this new approach is viable, but the author described myopes to 20.00D. Probably anyone from 14.00D to 20.00D would not need an IOL when the crystalline lens was removed.
Melvin Schrier, O.D.
Rancho Palos Verdes, Calif.
Where Do We Go Next?
In response to the article, Is Optometry Abandoning Its Roots? in the January issue of Review of Optometry, I ask: Where do we go next?
I would like to see housekeeping done within our profession. We have managed to create outstanding continuing education programs that are now accepted by most state boards without special permission. We need to move forward on licensure reciprocity. We are hindering ourselves as a profession and reducing economic opportunities by varying state licensure requirements.
I practice at the highest level of licensure in my state (Missouri) and I am able to treat glaucoma and prescribe oral medications, including Schedule III narcotics. There should be no reason why I cannot register and pay a licensure fee to practice in any other state. Yet to practice in some states, I would have to retake national boards and take the particular states boards.
Timothy Hug, O.D.
Kansas City, Mo.
Low Vision Driving in Florida
Congratulations on your article on driving and low vision (February 15, 2005), which is a subject that has been neglected for too long. However, the sidebar, Low Vision Driving Regulations in Certain States has errors that I would like to correct.
I refer to the regulations in Florida. A driver here may be licensed with 20/70 vision in either eye or both eyes with or without correction only if vision cannot be improved. If it can be improved, a corrective lens is required. Also, the minimum binocular horizontal field of vision required is 130 degrees, not 140 as your summary states.
I cannot respond to the requirements listed for other states, but I join you in urging optometrists to familiarize themselves with the requirements of their own state.
The article states that optometrists are required to report deficient drivers in Oregon and Pennsylvania, and that may be true. Although it is not required in Florida, anyone, including eye professionals but not limited to them, can report a driver who has inadequate vision, with complete anonymity, by using a special form obtainable from the Florida Division of Driver Licenses.
Robert Greenberg, O.D., F.A.A.O.
Tallahassee, Florida
