 |
Q:
A cataract patient sent to our practice also had diabetic macular edema (DME). How do I sort these issues out and to whom should I send the patient first, the retina specialist or the cataract surgeon?
A:
“Of critical importance for any patient being sent for cataract surgery consultation is a thorough exam, and in particular careful retinal evaluation,” says Jeffry Gerson, OD, of Grin Eye Care in Olathe, KS. In Dr. Gerson’s practice, patients have macular optical coherence tomography (OCT) done as part of the pre-op workup to find any subtle changes that may not have been noticed during the clinical exam. “These ‘hidden’ findings may become quite significant, and are especially important to document if your patient is considering a premium intraocular lens (IOL),” he adds.
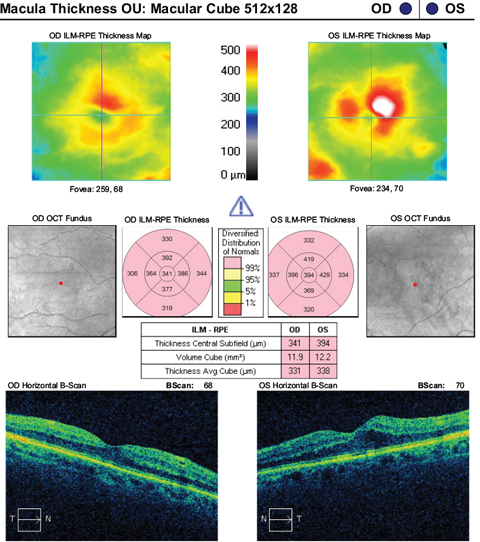 |
| This patient was only referred for cataract consultation but also ended up with a diagnosis of macular edema. |
At times, you or the cataract surgeon will want a patient to see a retinal specialist prior to undergoing cataract surgery for “clearance” if there is high myopia, lattice degeneration, diabetic macular edema or any other questionable pathology, Dr. Gerson continues.
“Epiretinal membranes are easily missed. While unlikely to be a reason to cancel cataract surgery, their identification is important in order to temper expectations,” says Dr. Gerson. “Macular edema, on the other hand, is a reason to cancel surgery, because it can be worsened by surgery and needs to be controlled before anything else is done.” In these cases, send patients to a retina specialist to further assess and treat the macular edema. Once the condition is stable and the patient is cleared by the retina doctor, then you are on safer ground to proceed with cataract extraction, Dr. Gerson says. “Of note, these patients often should be placed on nonsteroidal anti-inflammatory drug (NSAID) drops pre-operatively for longer than the average patient, and will likely be on the NSAID longer post-operatively than most patients in order to prevent later onset edema.”
Modern Knowledge
Historically, many believed cataract surgery would “speed up” conversion of dry age-related macular degeneration (AMD) to wet AMD, Dr. Gerson says. However, today we know this is not the case. “It is safe for patients with dry macular degeneration to undergo cataract surgery,” says Dr. Gerson. Just keep expectations realistic, especially about viable IOL options. For example, it probably would not be prudent to use multifocal IOLs that could affect contrast in a patient who already has reduced contrast sensitivity from AMD, Dr. Gerson adds. “As long as OCT is ‘dry,’ a retinal consult is not generally necessary, but may make sense in questionable cases.”
Since cataract surgery increases the risk of retinal detachment, practitioners should be sure to provide extra education for patients with high myopia, since they are already at a higher risk, says Dr. Gerson. While no preventative treatment applies to these cases, more frequent postoperative follow-up may be required. Additionally, practitioners should educate patients to call immediately if any symptoms are noted.
In one last scenario, a retina surgeon may request that the cataract be removed before they perform a procedure. “Two reasons for this would be better visualization for the retinal surgery, but also to see how much of the visual decline is due to cataract and how much is retina,” says Dr. Gerson. “If functional vision returns after cataract surgery, the more invasive procedure may not need to be performed.”
