A 29-year-old male was referred to the VA eye clinic for a red and painful left eye. He had noticed a burning sensation in his left eye 10 days earlier, which gradually worsened. His left eyelid became swollen one week after the onset of symptoms. He was diagnosed with conjunctivitis in the emergency department of a local hospital and was given Zymar (gatifloxacin 0.3% ophthalmic solution, Allergan) every six hours and told to follow up with an eye care specialist if the conjunctivitis did not improve. He had no previous history of injury or surgery to his eyes. There was a history of anisocoria and a fixed right pupil due to past traumatic brain injury (TBI); he also had a systemic history of dysarthria and vitamin D deficiency. He was not currently taking any medication and reported no known allergies.
Diagnostic Data
Uncorrected visual acuity was 20/20 OD and 20/40 OS with no pinhole improvement. Refraction was not attempted at the time. Vital signs were unremarkable. A fixed right pupil was detected with pupillary testing, but no reverse afferent pupillary defect was observed in the left eye. Restriction in upgaze was seen in the left eye during extraocular motility testing, and the patient reported seeing diplopia in upgaze. Visual fields were full and intact to finger confrontation in both eyes. The left conjunctiva was injected in all quadrants (Figure 1). Ptosis with mild eyelid edema was seen in the left eye. Retropulsion was equal in both eyes. No proptosis was observed in either eye. All other anterior and posterior segment findings were normal. There was no evidence of iritis, uveitis, vitritis, optic neuritis or pars planitis in either eye. Optic nerves were healthy and pink in color without pallor. Intraocular pressure (IOP) was 15mm Hg OD and 13mm Hg OS.
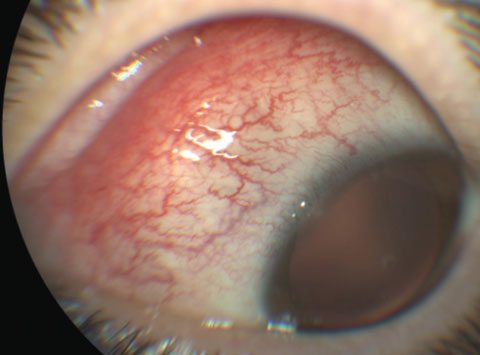 |
| Fig. 1. Nasal and superonasal conjunctival injection. |
Given the painful and limited gaze findings, a tentative diagnosis of preseptal cellulitis of the left eye was made, and stat computed tomography (CT) of the orbit was ordered to rule out any orbital involvement, including orbital cellulitis and orbital abscess. The patient was started on Tobradex (tobramycin and dexamethasone ophthalmic ointment, Alcon) one drop QID for 10 days in the left eye for possible nonspecific conjunctivitis. He was also started on Augmentin (GlaxoSmithKline) 875mg BID for 10 days. The patient was instructed to sleep with his head elevated 10 to 20 degrees and to apply a cool compress on the left eye for five to 10 minutes twice daily. He was scheduled to return in three to five days for follow-up.
A radiologist at the VA medical center reviewed the stat CT of the orbit with contrast. The report stated there was a 9mm by 19mm ill-defined soft tissue mass in the superomedial orbit exerting mass effect on the adjacent globe, along with some diffuse scleral thickening and mild enlargement of the lacrimal gland (Figure 2). According to the radiologist, the presentation on CT scan was most indicative of orbital pseudotumor. Lymphoma could be considered in the appropriate clinical setting, while infection was less likely, according to the report.
We referred the patient to our ophthalmology department the same day for further evaluation. Ocular protrusion was measured at 14mm OD and 16mm OS at base of 88 using a Hertel exophthalmometer. All other clinical findings remained unchanged. Baseline blood tests were ordered, and mild leukocytosis was detected with CBC; otherwise, all lab results were negative and within normal limits.
| Table 1. Differential Diagnosis1-3 | ||
| IOIS | Orbital Cellulitis | Thyroid Eye |
| Severe pain that is worse on eye movement. | Pain is severe. | Pain is mild. |
| Usually unilateral, acute onset. | Unilateral, acute onset. | Commonly bilateral with asymmetry; gradual, subacute onset. |
| Vision is usually normal; can be affected early. | Vision is affected at late stage, unless fungal | Vision usually affected in later stage. |
| Ocular movement is restricted in field of inflamed muscle. | Ocular movement restricted. | Ocular movement restricted. |
| Ptosis and eyelid swelling. | Eyelid swelling. | Lid retraction and lag. |
| Imaging shows muscle enlargement and extension to orbital fat. | Imaging shows sinus disease, bony erosion and venous thrombosis. | Imaging shows muscle enlargement, tendons spared, no extension to orbital fat. |
| Rapid response to steroids. | Fever and elevated WBC present; history of sinus infections, dental problems and trauma. | Abnormal thyroid function or immunoglobulin studies. |
Diagnosis
Based on the clinical presentation, orbital CT and lab results, the patient was diagnosed with orbital inflammation of the left eye by the ophthalmologist, most likely due to idiopathic orbital pseudotumor, also known as idiopathic orbital inflammatory syndrome (IOIS). Orbital cellulitis and thyroid eye disease are most often confused with IOIS, but in this case, diagnosis was not precluded by a misinterpretation of radiologic findings.1-3
Treatment and Follow-Up
The patient was started on oral prednisone 60mg daily, since the orbital inflammation was most likely due to orbital pseudotumor.
Other treatment options were presented to the patient, and he declined intravenous antibiotic therapy at the hospital because he had young children at home. Oral antibiotic therapy was not considered. A biopsy was recommended if the orbital mass persisted without resolution.
Two days after starting prednisone, the patient reported subjective overall improvement in his left eye. When he returned to ophthalmology for his two-day follow up, his uncorrected visual acuity was 20/20 OD, 20/30+2 OS with no pinhole improvement. He still had pain with eye movement, but symptoms of diplopia had improved. The patient’s left eye still had limited upgaze and ptosis was present secondary to eyelid edema. The conjunctival injection showed slight improvement compared with its initial presentation. The patient was to continue taking 60mg prednisone daily and return to ophthalmology in one week.
Unfortunately, the patient missed his two subsequent appointments. When contacted regarding the condition of his left eye, he said it was doing well. The patient never returned to either the eye clinic or ophthalmology; but, when reviewing his records, we came across an encounter note by a radiologist who saw the patient 10 months later for a CT of the head. The note stated that the patient’s right pupil was fixed and non-reactive, his left pupil was reactive and all eye movements were normal.
Discussion
IOIS is a diagnosis of exclusion.1,4-7 In 1905, researchers described the condition as an “orbital mass clinically mistaken for a neoplasm that was histologically inflammatory.”1 IOIS is a benign, non-infectious and non-neoplastic clinical syndrome that displays a nonspecific inflammatory process.1,4-6,8 It is an inflammation of the orbit with no known local or systemic etiology, and often occurs between the third and fifth decades of life, without any gender or race preferences. The condition makes up 5% to 8% of all orbital lesions and 16% of all cases of unilateral ptosis in adults.1,4-7 IOIS occurs in 6% and 17% of the pediatric population; 45% these cases present bilaterally.1,4-9 It is the third most common orbital disease behind Graves’ disease and lymphoproliferative disorders (LPDs).1,5,10
Orbital pseudotumor is divided into four histopathological subtypes:
- The granulomatous form contains histiocyte infiltration and multinucleated giant cells.
- The vasculitic subtype requires a work-up for collagen vascular disease (Wegener’s granulomatosis, polyarteritis nodosa).
- The eosinophilic form usually occurs when toxic granular proteins are released into the orbital connective tissue.
- The sclerosing form is a rare type that has histologic findings similar to other systemic fibroproliferative diseases such as retroperitoneal fibrosis. It is made mostly of dense fibrotic connective tissue with a few inflammatory infiltrates.1,2,6,9 Sclerosing-associated orbital inflammation, however, is now considered to be a separate disease entity.10
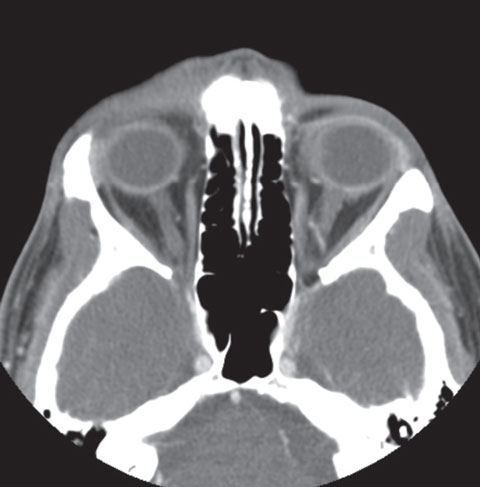 |
| Fig. 2. CT of orbit, ear and fossa without contrast. |
While the etiology is unknown, three possible causes exist: upper respiratory infections, immune-mediated and trauma.1,2,4,5,11 Recent literature suggests IgG4-associated orbital inflammation may also cause the condition.8,11,12
IOIS is usually unilateral, and its acute onset may occur within hours or days.1,4-6,13 The onset can also be subacute (weeks), chronic (months) or recurrent, the last of which occurs more often in cooler months.1,13 Signs and symptoms of IOIS include:
- Diplopia, pain and photophobia
- Proptosis and eyelid edema
- Conjunctival chemosis and injection in the affected eye1,7
- Lack of fever
- Ocular motility restrictions and cranial nerve palsies (III, IV, V1/V2, VI)
- Palpable orbital mass and lacrimal gland enlargement
Less common signs and symptoms include uveitis, elevated IOP, optic nerve swelling/atrophy, retinal edema, choroidal folds, hyperopic shift, posterior scleritis and decrease or loss of vision.1,4-6,9,10,13,14
Diagnostic Imaging
Magnetic resonance imaging (MRI) with contrast and CT are the ideal evaluation tools for orbital pseudotumor.1,4,8,13 The images will show enlarged muscles and tendons, as well as inflammatory infiltrates.1,4 Hematologic work-up should include:
- Erythrocyte sedimentation rate (ESR)
- Complete blood count (CBC)
- Blood urea nitrogen (BUN)
- Creatinine and Fasting blood sugar (FBS)
- Angiotensin-converting enzyme (ACE)
- Serum protein electrophoresis (SPEP) and Anti-neutrophil cytoplasmic antibody (ANCA)
- Anti-double stranded DNA (anti-ds DNA)
- Electrolytes and a rapid plasma reagin test2,6
Biopsy is usually not indicated unless steroid treatment yields a minimal response, imaging studies show persistent abnormalities, or if the patient presents with progressive neurological deficits.3,8,15
Treatment
IOIS is primarily treated with oral corticosteroids.1,3-5,8,9,13,15 The standard treatment regimen, which typically elicits a quick amelioration of IOIS symptoms, is prednisone 60mg to 100mg daily for two weeks, then a slow taper over weeks to months.3,6,9,13,16 Pain and proptosis may resolve quickly—in as little as 24 to 48 hours.3
Radiation therapy is an alternative treatment option if a patient is unable to tolerate steroid treatment, or is steroid resistant.
Immunosuppressant agents such as methotrexate, cyclophosphamide, azathioprine, cyclosporine and mycophenolate have also been used as treatments for IOIS with some documented success.1-6,13,15,17 Rituximab, a monoclonal antibody for treatment of B-cell lymphomas, chronic lymphocytic leukemia and rheumatoid arthritis, is emerging as an additional treatment option for IgG4-associated orbital inflammation, according to recent studies.8,12,18 Rituximab appears to be effective in treating patients with recurring orbital inflammation and those who were treated unsuccessfully with steroids and immunosuppressants.8,12,18
Conclusion
Because IOIS is an idiopathic inflammation of the orbit, it is a diagnosis of exclusion. Imaging studies are a key tool for evaluating and diagnosing this syndrome. Blood work will help rule out any potential systemic conditions. Prednisone remains the primary mode of treatment for IOIS Radiation, immunosuppressants and rituximab are also treatments to consider for this ocular condition. Follow the steps to an appropriate diagnosis and implement the right treatments to yield positive outcomes for your patient’s ocular health.
Dr. Yee is a staff optometrist at the W. G. Bill Hefner VA Medical Center. Her clinical interest is in ocular disease.
|
1. Zerilli TC, Burke CL. Orbital pseudotumor after an upper respiratory infection: a comprehensive review. Optometry. 2010;81:638-46. 2. Espinoza G. Orbital inflammation pseudotumor: etiology, differential diagnosis and management. Curr Rheumatol Rep. 2010;12:443-7. 3. Jacobs D, Galetta S. Diagnosis and management of orbital pseudotumor. Curr Opin in Ophthalmol. 2002;13(6):347-51. 4. Guerriero S, Leo ED, Piscitelli D, et al. Orbital pseudotumor in a child: diagnostic implications and treatment strategies. Clin Exp Med. 2011;11:61-3. 5. Deaner J. September 2014 Wills eye resident case series-diagnosis and discussion. Review of Ophthalmology. 2014;21(9):67-9. 6. Swamy BN, McCluskey P, Nemet A, et al. Idiopathic orbital inflammatory syndrome: clinical features and treatment outcomes. Br J Ophthalmol. 2007;91:1667-70. 7. Cooney NL. Orbital pseudotumor. Int J Emerg Med. 2009;2:263. 8. Teke TA, Kaman A, Metin O, et al. Idiopathic orbital inflammation in a child mimicking orbital cellulitis. Clinical Pediatrics. 2015:1-3. 9. Mulvihill A, Smith CR, Buncic JR. Pediatric orbital pseudotumor presenting as a painless orbital and periocular mass. Canadian Journal of Ophthalmology. 2004;39(1):77-9. 10. Pakdaman M, Sepahdari AR, Elkhamary SM. Orbital inflammatory disease: pictorial review and differential diagnosis. World Journal of Radiology. 2014;6(4):106-15. 11. Oles K, Szczepanski W, Skladzien J, et al. IgG4-related inflammatory orbital pseudotumors-a retrospective case series. Folia Neuropathologica. 2015;53(2):111-20. 12. Carbone T, Montes RA, Andrade B, et al. Orbital pseudotumor: uncommon initial presentation of IgG4-related disease. Case Reports in Rheumatology. 2015;1-4. 13. Muqtasid AK, Ali G, Ishrat HD, et al. Orbital pseudotumor. Oman J Ophthalmol. 2009;2(2):96-9. 14. Turkoglu R, Balak N. Atypical presentation of orbital pseudotumor with visual loss as an initial manifestation. J Clin Neurol. 2011;7(1):50-2. 15. Matthiesen C, Bogardus CJ, Thompson SJ, et al. The efficacy of radiotherapy in the treatment of orbital pseudotumor. Int J Radiation Oncology Biol Phys. 2011;79(5):1486-1502. 16. Shen T, Chen J, Lin J, et al. Concomitant idiopathic orbital inflammatory pseudotumor and thyroid-associated ophthalmopathy. Journal of Craniofacial Surgery. 2015;26(6):479-81. 17. Falcini F, Simonini G, Resti M, Cimaz R. Recurrent orbital pain and diplopia in a 12 year old boy. Ann Rheum Dis. 2002;61:93-4.18. Suhler EB, Lim LL, Beardsley RM, et al. Rituximab therapy for refractory orbital inflammation: results of a phase ½, dose-ranging, randomized clinical trial. JAMA Ophthalmol. 2014;132(5):572-8. 19. Chen T, Figueira E, Lau, OCF, McKelvie PA, Smee RI, Dawes LC, Agar A, Wilcsek G, Francis LC. Successful “Medical” Orbital Decompression with Adjunctive Rituximab for Severe Visual Loss in IgG4-Related Orbital Inflammatory Disease with Orbital Myositis. Ophthal Plast Reconstr Surg. 2014; 30(5): 122-125. 20. Hiraga A, Kuwabara S. Recurrent Alternation Orbital Inflammation. Journal of the Neurological Sciences. 2015;357:288-9. |
