 |
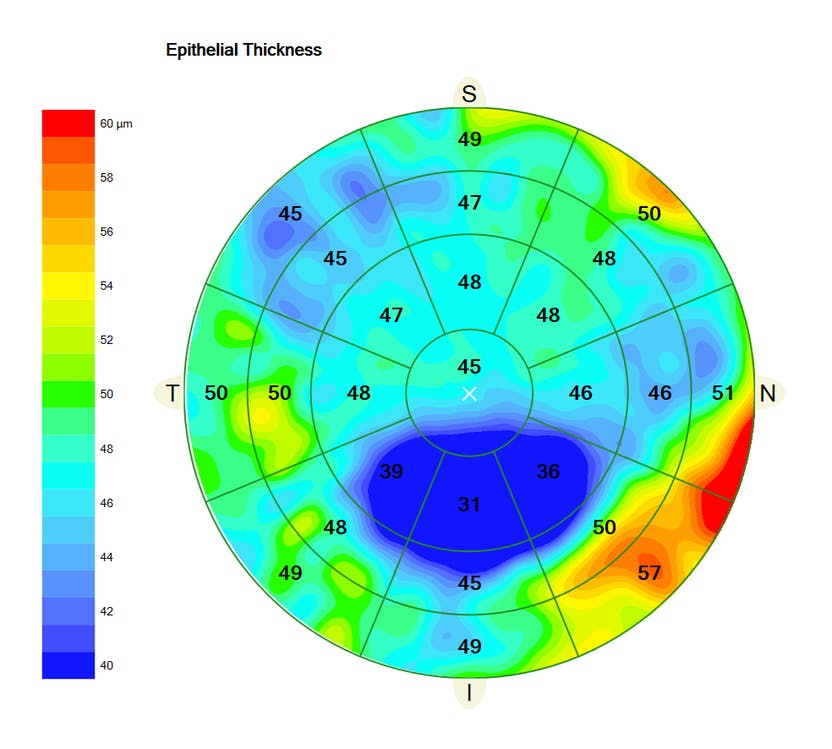
Patients with different types of astigmatism (characterized by the orientation of the steepest corneal meridian) had varying epithelial thicknesses in this study. Photo: Carl Zeiss Meditec. Click image to enlarge. |
There are many uses for corneal epithelial thickness mapping, such as keratoconus screening and dry eye assessment. It also plays a crucial role in corneal laser refractive surgery; for example, in patients receiving transepithelial photorefractive keratectomy, an asymmetric epithelial thickness profile could result in refractive inaccuracy. A recent study sought to develop a reference for epithelial thickness profiles in various types of corneal astigmatism by examining individuals with no ocular surface disorders.
The cross-sectional study included 154 left eyes of 154 patients, ages 18 to 40, who presented for refractive surgery. Included patients had no history of ophthalmic surgery, comorbidities, topical or systemic drug use, allergy or other conditions that would have an effect on the ocular surface. The patients were also required to abstain from contact lens wear for at least three months.
Corneal topography and epithelial thickness mapping by anterior segment OCT was performed on each patient. The researchers explained, “Corneal astigmatism was classified based on the orientation of the steepest corneal meridian (with- and against-the-rule (WTR and ATR) and oblique) and the amount (low, moderate and high).” They determined that WTR, oblique and ATR astigmatism were present in 40%, 31% and 29% of eyes in the study, respectively.
They found that in patients with any type of astigmatism, the mean epithelial thickness was greater along the 180° meridian and thinner along the 90° meridian. In addition, they added that there was “no significant difference in mean thickness among different amounts of WTR astigmatism. In addition, there was no statistically significant difference in thickness along different meridians separately in low, moderate and high astigmatisms.”
However, the researchers observed that the difference along the 180° and 90° meridians for ATR astigmatism was statistically significant and that “there was a statistically significant difference in thickness in different types of astigmatism separately for each meridian so that the highest and lowest thicknesses were seen for ATR and oblique astigmatisms, respectively.”
In conclusion, the researchers found no difference in epithelium thickness between the various amounts of astigmatism, but they did find a few differences between the various types included in this study. “A thicker epithelium along the horizontal meridian in ATR may point to the surface regularizing functions of the epithelium to create a regular and smooth surface, but thickness assessment along the different meridians in oblique and WTR showed no curvature-dependent changes,” they concluded.
Sedaghat M-R, Momeni-Moghaddam, H, Azimi A, et al. Comparison of epithelial thickness mapping in normal corneas with different types of astigmatism. Optom Vis Sci. February 23, 2022. [Epub ahead of print]. |
