 |
Q: I have a seven-year-old white male who presented with a rather unusual dry eye symptoms. His cornea and conjunctiva stained in both eyes with lissamine green. Standard treatments for dry eye have failed. Though I’ve considered the typical masqueraders, I have failed to identify a cause. Any thoughts on what this is?
A: “In all patients, including children, it is critical to obtain a review of systems, including topical and oral medications to rule out any systemic causes of ocular surface disease,” says Melissa Barnett, OD, of the UC Davis Eye Center in California. She recommends the patient undergo a general physical exam including laboratory work when indicated; he should also be asked about lifestyle activities, including electronic device use, that could contribute.
Jeffrey J. Walline, OD, PhD, associate dean for research at Ohio State University, agrees, pointing out a number of atypical reasons for a presentation like this in children and adolescents. “Juvenile rheumatoid arthritis may be considered as a relatively common cause of dry eye in children,” he says. “Does the child appear nutritionally healthy? A vitamin A deficiency could lead to dry eye issues. Have you considered diabetes? Although the symptoms of diabetes are relatively obvious, the appropriate questions may not have been asked previously.”
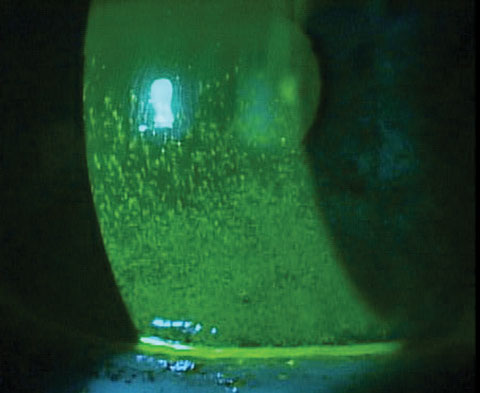 |
| Significant corneal staining in a patient with rheumatoid arthritis. Photo: Mile Brujic, OD. |
Use of some medicines like antihistamines, video game use, and sleeping with the eyes open are also potential causes. The sleeping habit in particular is likely to cause a linear pattern of staining, Dr. Walline notes, adding that most of these can be determined by recording a thorough patient history.
Mile Brujic, OD, suggests examining the patient’s physical features for further signs. “Make sure to assess for any anatomical anomalies, specifically looking for loose lids or incomplete blinks,” he says. “Observe the patient to make sure there is not an ocular allergy that may be causing irritation to the eye from itching.” Compulsive eye rubbing is a clear sign of a possible allergy.
Additionally, Dr. Brujic suggests ruling out the possibility of mucus fishing syndrome, and paying “particular attention to the lash margin to [eliminate] blepharitis, which at times can be aggressive in young children.”
Dr. Barnett agrees, adding that meibomian gland expression is helpful in evaluating the quality of the meibomian glands, and examination of the palpebral conjunctiva, bulbar conjunctiva and cornea can indicate presence of allergies. She suggests implementing dietary supplementation with omega-3 and omega-6 fatty acids and reducing consumption of fried or fatty foods. Fitting the patient with scleral lenses is also an option if the practitioner deems them necessary.
On the medical side, more atypical possibilities like Riley-Day syndrome and celiac disease should also be ruled out. These can be identified via corneal anesthesia with lack of tear reflex present and an evaluation of serum vitamin A levels, respectively.