DEWS II: Redefining Dry EyeFollow the links below to read the other articles from our coverage of TFOS DEWS II: A Definitive Decade for Dry Eye What Does “Dry Eye” Mean Today? |
This article covers the following TFOS DEWS II reports:
II. Sex, Gender and Hormones
IV. Tear Film
V. Pain and Sensation
VI. Pathophysiology.
Research on dry eye has flourished over the last decade. While the original TFOS DEWS report included a section on research, it spanned just 14 pages with 216 references. TFOS DEWS II cites over 5,000 references in total and breaks the topic down into several research-specific subsections, such as pathophysiology; sex, gender and hormones; the tear film; and pain and sensation.
DEWS II provides unparalleled access to the global expert consensus on today’s understanding of the disease and the ocular structures it affects. Here’s a look at how they can impact your clinical acumen when treating patients with dry eye.
Pathophysiology
While the original TFOS DEWS report of 2007 did not include a separate pathophysiology section, the TFOS DEWS II report dedicates 75 pages to fully exploring the current understanding of the mechanisms of action behind DED. With 1,220 references, this section provides a comprehensive look at the mechanisms involved in the creation and perpetuation of DED.
The bottom line: “DED is initiated by desiccating stress and perpetuated by a vicious circle of ocular surface inflammation.” [VI, 3, p. 442]
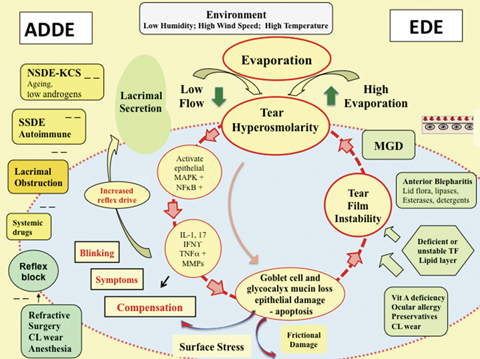 |
Fig. 1. THE VICIOUS CYCLE OF DRY EYE DISEASE. The core mechanism of DED is tear hyperosmolarity, the hallmark of the disease. It damages the ocular surface both directly and by initiating inflammation. The cycle of events is shown at the center of the figure. Adapted and reprinted from Ocular Surface (2017) 441–515, Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report, p. 460, © 2017, with permission from Elsevier. |
“The concept of the vicious circle has been reinforced over the past 10 years with evaporation, influenced by the environment, being the source of tear hyperosmolarity,” Anthony Bron, FRCOph, lead author of the Pathophysiology section, explained during a special session at this year’s ARVO meeting. “We know that hyperosmolarity causes pain directly, induces inflammatory signaling, epithelial cell death, MMP production, glycocalyx changes and it amplifies the process of mitosis, whereby the release of extracellular DNA activates a multicomponent inflammatory response of the ocular surface,” said Dr. Bron.
GUIDE TO NOTATIONThis supplement summarizes the 10 subcommittee reports that comprise TFOS DEWS II, published in the July 2017 Ocular Surface. The top of each article lists the reports discussed therein. Readers interested in more detail are encouraged to seek out the full text. For easier exploring, key points cite the relevant source by report, paragraph and page number. As you read the ensuing articles, look for TFOS DEWS II citations in this notation: [report #, paragraph #, page #] Example: [IV, 2.3, p. 372] |
This general thesis was just the starting point, however. The subcommittee further described the mechanics that maintain the tear film and what happens when homeostasis is lost—namely, exposure of the ocular surface to damaging desiccation. [VI, 3, p. 442]
The central mechanism at play, they summarize, is evaporative water loss leading to hyperosmolar tissue damage. [VI, abstract, p. 441] This central mechanism initiates changes that lead to evaporative dry eye (EDE)—“where tear hyperosmolarity is the result of an excessive evaporation from the tear film in the presence of normal lacrimal function”—and aqueous-deficient dry eye (ADDE)—“where hyperosmolarity results from a reduced lacrimal secretion in the presence of a normal rate of tear evaporation.” [VI, 5.1, p. 455] From here, the vicious circle takes over, perpetuating ocular surface issues that exacerbate signs and symptoms and often morphs the condition into a hybrid form of dry eye (Figure 1).
Because of this complex interplay between various forms of DED, the subcommittee recommends retaining the terms EDE and ADDE “to describe the initiating basis of a dry eye, but it should be recognized that with progression any form of DED may take on additional evaporative features.” [VI, 5.1, p. 456]
Also, while studying what is known about the mechanisms of dry eye, the researchers realized that not all patients who show corneal staining have DED, and conversely, those with staining might have conditions other than dry eye.
“A portion of normal corneas show a little staining, so no staining is not the default in the normal eye,” Dr. Bron said at ARVO. This provides more support for the inclusion of the normal eye in the updated classification system.
The lengthy review also highlighted areas lacking proper research, and Dr. Bron boiled down the subcommittee’s biggest findings and recommendations: “We need new methods to measure the tear evaporation and osmolarity at the tissue level. We should recognize that the absence of corneal staining is not the normal default, and that hybrid dry eye states are very prominent.”
Sex, Gender and Hormones
With 994 references, this report provides a comprehensive look at a body of literature that spans centuries, focused on the role sex, gender and hormones play in regulating the ocular surface and disease prevalence and progression. All three are integral and affect a patient’s health, disease risk, diagnosis and progression, and even perceptions about health, the authors assert. [II, 1, p. 285]
“Our eye health is affected by various hormones,” says Juan Ding, OD, PhD, a coauthor of the report. “When we treat dry eye disease, it is helpful to keep in mind that the patient’s overall well-being may be a reason for their dry eye, and that we are not just treating the eye, but are actually treating the person by taking into consideration potential systemic causes of dry eye disease.”
“Does sex matter? Yes, every self has a sex,” said David A. Sullivan, PhD, the TFOS DEWS II report organizer, during the ARVO special session. “It’s an important basic human variable, especially considering that the occurrence, frequency and severity of diseases may vary between males and females.”
For starters, women in the United States are as much as 70% more likely to be diagnosed with DED than men, and the literature suggests women experience a greater impact of DED on visual quality indicators and on tasks requiring sustained visual attention. [II, 2.2.1, p. 286; II, 2.2.2, p. 287]
The research also shows a significant sex-related difference in ocular structures, including the lacrimal glands, meibomian glands, cornea, conjunctiva, nasolacrimal duct and tear film—all of which the subcommittee members speculate may contribute to the increased prevalence of DED in women. [II, 2.3, p. 288]
“There is a huge body of evidence to support that female sex is a risk factor for dry eye,” says Sruthi Srinivasan, PhD, BS Optom, a coauthor of the report. “Are we being proactive about this in our practice? This report should make clinicians and researchers think about using different dry eye diagnostic tests and management techniques and strategies while examining men vs. women.”
While most literature focuses on the biological differences between sexes, some highlights the role gender plays as well.
“Sex is not the same as gender,” Dr. Sullivan emphasized at ARVO. “Sex is distinguished as males and females based on biological characteristics, and gender is first linked to socially constructed characteristics such as roles, behaviors and expectations related to being male or female.”
“The literature abounds with examples of gender-based health disparities in access to care, care-seeking behavior (particularly in women in developed countries), communication with health care providers, service utilization and health outcomes around the world,” according to the report—and all of these may apply with DED. [II, 4.1, p. 314]
Current research makes clear the importance of sex, gender and hormones on a patient’s health and health care experience; still, the study authors also identified a number of shortcomings within the literature and recommend researchers work to remove barriers, including ethical, financial, sociological and scientific considerations. [II, 2.1.1, p. 286]
The Tear Film
Perhaps the most important factor in the study of dry eye is the tear film, as “DED is characterized by loss of tear volume, more rapid break-up of the tear film and increased evaporation of tears from the ocular surface.” [IV, 1, p. 369]
Understanding the rapid break-up of the tear film demands a firm knowledge of the structure itself—not an easy task. While most researchers are comfortable with the many components of the tear film, such as lipids, proteins, mucins and electrolytes, how they all interact is still under investigation. The TFOS DEWS II Tear Film subcommittee emphasized that holding firm to the three-layer model of the tear film “has generally limited novel perspectives that might lead to a clearer understanding of the dynamics, structure and function of the tear film and the changes that occur to cause dry eye.” [IV, 1, p. 369] Instead, researchers and clinicians should see the tear film for what it is: “a dynamic functional unit with different compartments.” [IV, 1, p. 369–70] The committee described a lipid layer covering and integrated with a complex mixture of aqueous, mucins and proteins, all of which work together to maintain tear film and ocular surface homeostasis (Figure 2).
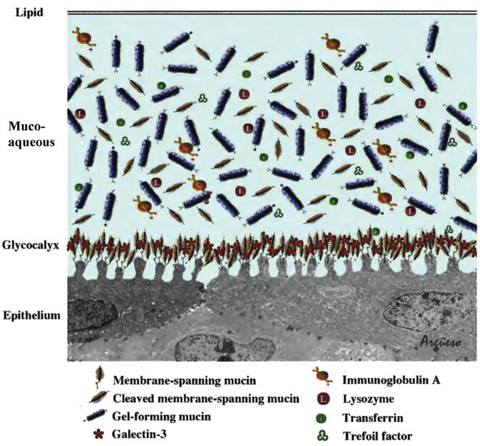 |
Fig. 2. The tear film structure showing the mucins and galectin of the glycocalyx, soluble mucins and proteins in the mucoaqueous layer and the surface lipid layer. Reprinted from Ocular Surface (2017) 369-406, Willcox MDP, Argüeso P, Georgiev GA, et al. TFOS DEWS II tear film report, p. 383, © 2017, with permission from Elsevier. |
A closer look at the lipid layer specifically helped to highlight both its importance and the long research road ahead to understand it fully. For one thing, the lipid layer lowers the tear surface tension, sustaining the tear film’s high area-to-volume aspect ratio, the report states. [IV, 3.3, p. 378] “The tear film lipid layer was clearly important in stabilizing the tear film, as degradation increases the surface tension; but interestingly, supplementation to delipidated tears with meibum lipids does not seem to be able to restore the lost surface tension,” explained Mark Willcox, PhD, lead author of the Tear Film subcommittee report, during the ARVO special session. This suggests normal surface tension may rely on not just lipids, but possibly proteins and glycoproteins from the mucoaqueous layer, the report says. [IV, 3.3, p. 378]
In addition, despite varying hypotheses to explain tear evaporation suppression—with the lipid layer variously credited with some, all or none of the effect—the researchers finally concluded that “all tear film key constituents may contribute to increased evaporative resistance.” [IV, 3.1, p. 376–377]
So far, it’s clear tear film osmolarity increases in DED, and changes to proteins and mucins can be used as biomarkers, but more research is still needed to fully understand the mechanisms at play within the tear film.
“Still, the most useful, from a clinical perspective, methods for diagnosing dry eye in the clinic are measuring osmolarity and stability of the tear film,” Dr. Willcox said in a correspondence. “These, coupled with Schirmer I, questionnaires such as the Ocular Surface Dryness Index and examining the meibomian glands, facilitate a good diagnosis.”
To aid in further studies, the report authors recommend researchers be meticulous with terminology to avoid confusion and misrepresentation.
For example, the assumption that tear osmolarity is approximately 302mOsm/L is often acceptable, but technically that number is the value only for tears from the lower tear meniscus. [IV, 1, p. 370] It may represent the overall osmolarity of the ocular surface, but no evidence supports that hypothesis yet. A more careful approach to terminology could lead to more precise data and better findings.
“Newer methods that measure aspects of the tear film, such as changes in the concentration of proteins, lipids and mucins, are being developed, but are not at the stage of clinical testing,” Dr. Willcox continued. “It is probable that future testing will incorporate changes in, for example, a range of proteins and this should improve the specificity and sensitivity of tests.”
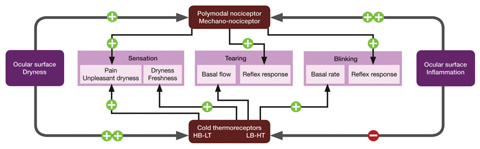
SPOTLIGHT ON PAIN AND SENSATION“We insist on the concept that dry eye symptoms and sensations are a form of pain,” said lead author Carlos Belmonte, MD, PhD, during the ARVO special session. Moving forward with this concept in mind, the Pain and Sensation subcommittee took a closer look not only at the neurons that innervate the ocular surface but how they respond to “mechanical forces, noxious chemicals and to low temperatures and the change in osmolarity,” said Dr. Belmonte.
Adapted and reprinted from Ocular Surface (2017) 407-440, Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pain and sensation report, p. 423, © 2017, with permission from Elsevier. Corneal sensory neurons are broken down into three categories: polymodal nociceptors, specific mechano-nociceptors and cold thermoreceptor neurons. While polymodal nociceptors respond to chemical, mechanical and thermal stimuli and become sensitized by inflammation, mechano-nociceptors only respond to mechanical forces. [V, 8, p. 430] The most important neurons in the pathology of dry eye, researchers suspect, are cold thermoreceptors, which discharge continuously with normal eye surface temperature and increase or decrease the firing frequency based on cooling or warming, respectively. These neurons also seem to be sensitive to changes in osmolarity, leading the authors to suggest that “cold-sensitive fibers contribute to the reflex control of basal tear production and blinking.” [V, 8, p. 430]
The inflammation in DED caused by reduced tear secretions may sensitize polymodal nociceptors and mechano-nociceptors, while depressing cold thermoreceptor activity, they found. [V, 8, p. 430] But at the same time, the literature shows sensitization of nociceptor fibers is minor in DED, while a prominent and abnormal increase in cold thermoreceptor nerve activity occurs that parallels the morphological changes in corneal innervation. [V, 8, p. 430] But knowing the science behind pain pathways can only take you so far in your clinical practice, because “the complex pain and discomfort experience suffered by dry eye patients is very variable,” Dr. Belmonte said. The subcommittee recommends clinicians rely on pain questionnaires to help characterize their patients’ discomfort, in addition to tear component testing and in vivo confocal microscopy to better view the nerve endings affected by DED. More studies are needed in this emerging area of dry eye disease, they conclude. |