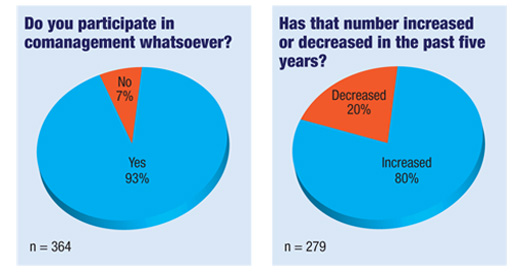
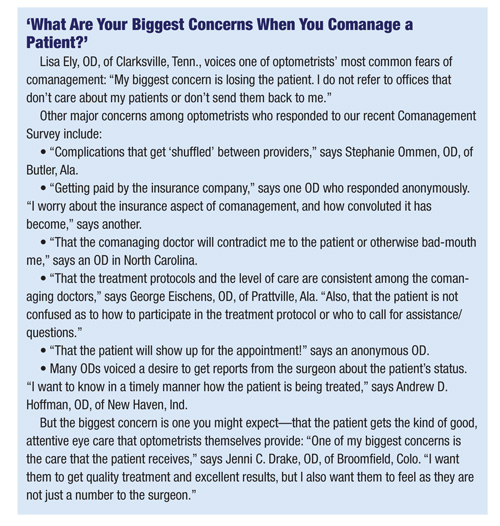
Even with these concerns, optometrists are comanaging more patients with surgeons, specialists and other ODs. Specifically, 93% of ODs who answered our recent Comanagement Survey say they participate in some form of comanagement at least once a month. And 80% report that the number of patients they comanage has been increasing during the past few years.
 |
We found that the number of patients that individual optometrists comanage varies widely—from less than one patient per month to upwards of 400 (according to an OD in a referral center). But, if we separate out those ODs who work in referral centers and in large OD/MD practices, as well as those ODs who don’t comanage at all, then we find that the “average” OD comanages about 12 patients a month (actually 12.33, but you can’t bill on one-third of a patient). Of that number, our respondents comanaged an average of 11 patients per month for surgical procedures (again, varying from zero to up to 50), and comanaged about one or two patients a month (ranging from zero to 30) for non-surgical treatments (such as for vision therapy or low vision).
 |
More Patients, More Acceptance
There are several reasons for the increase in comanagement. But here are the two biggest ones:• More cataract patients. You’ve heard it a million times before: the Baby Boomers are coming! Guess what? They’re finally here. “The average age of my patients is increasing the longer I am in practice, which has resulted in more cataract surgery and glaucoma comanagement,” says Mark Snyder, OD, of Hyannis, Mass. Indeed, a recent study from the Mayo Clinic found that the number of cataract procedures has increased steadily for more than three decades, and reached record levels in 2011.1 The study also found that people are getting the procedure at a younger age, and are frequently having it done on the second eye sooner.
• Surgeons are more accepting. Although the number of cataract patients is increasing, the number of ophthalmic surgeons is not. That may be one reason why an increasing number of surgeons are lowering their resistance to optometric comanagement. Or, it could be a sign of the times—more surgeons have seen that it works and have accepted the idea. “I have comanaged refractive surgery and cataracts for more than 20 years,” says Dawn Rakich, OD, of San Antonio. “Our new surgeon has allowed one-day post-ops for cataracts now, so postoperative care is passed off to me immediately after surgery.”
Not all comanagement is growing, though. “We’ve increased the number of cataract surgery patients, but we’ve seen a significant decrease in the number of LASIK patients,” says Paul Heersink, OD, of Monte Vista, Colo. LASIK procedures began a decline even before the economy bottomed out in 2009, and still haven’t recovered.
OD-to-OD Comanagement
We also asked, “Do you ever comanage patients with another optometrist?” Responses were almost evenly divided: 52% say they do, 48% say they don’t. Some ODs responded with equivalent of a shrug: “Why would I do that? What is the added value for the patient?” one optometrist asks.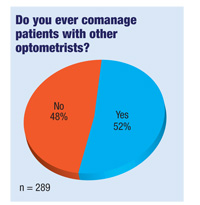 |
 |
 |
| |
The survey also asked whether optometrists send patients to an optometric referral center for secondary or tertiary care. About 27% say they’ve done this. Many of the rest answered that they don’t have one nearby—or that they’ve never even heard of such a thing. (To explain: An optometric referral center is an optometrist-owned multispecialty eye care practice. It employs ODs and MDs but handles no primary care, only secondary or tertiary care. The Omni Eye Centers are a prime example. “Every patient is sent in by a referring optometrist and returned to the referring optometrist,” responds an OD who works at one such center.)
Typical Situations
Although more optometrists are participating in comanagement in general, that doesn’t tell the whole story. ODs are also handling more medical eye care themselves. For instance, 67% say they will manage a typical glaucoma patient on their own, while 30% will refer to an MD. That percentage has nearly flip-flopped since our Comanagement Survey in 1998. Back then, 64% of optometrists said they send their typical glaucoma patient to an MD, and only 46% said they manage the patient themselves. Meanwhile, slightly fewer ODs handle vision therapy and low vision themselves, as compared to 1998. They’re now more inclined to send those patients to an optometric colleague who can provide those specialized services.When a Referral Goes South
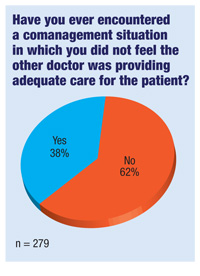
Our survey also found that 38% of optometrists had a problem in which the comanaging doctor did not seem toprovide adequate or appropriate care. How do ODs handle this? In many cases, ODs simply stop referring patients to that doctorand send the patient to a different surgeon or provider instead. Sometimes, they just take over the care themselves. But this non-confrontational approach may not be the best. If you’re faced with such a situation, don’t be afraid to call your MDs on it—literally. “I picked up the phone, called and talk to them about it,” says Marla L. Moon, OD, of State College, Pa. “If they changed their ways and improved, I continued to refer. If not, they stopped getting referrals from me.”Similarly, “I made direct contact on each specific patient to discuss the care that was being provided,” says R. Ted Watson, OD, of Greenville, NC. “In each case, the comanagement dialogue was beneficial for all concerned.”1. Gollogly HE, Hodge DO, St Sauver JL, Erie JC. Increasing incidence of cataract surgery: population-based study. J Cataract Refract Surg. 2013 Sep;39(9):1383-9.
