 |
Q:
I recently saw a patient with a significant Pseudomonas ulcer in which the edge had reached the limbus. The corneal specialist added an oral antibiotic. Is this necessary, and what’s the best option for treatment?A:
“A Pseudomonas ulcer that spreads to the limbus is a true, globe-threatening ocular emergency,” Eric Donnenfeld, MD, national medical director of TLC Laser Eye Centers, says. “Once Pseudomonas ulceration reaches the limbus it has the potential to extend into the sclera.”
Additionally, a scleral abscess is “much more unresponsive to treatment than a corneal ulceration and often requires enucleation,”
Dr. Donnenfeld adds, suggesting this is why “most corneal specialists are extremely aggressive in treating infections near the limbus.”
“While Pseudomonas keratitis can be very aggressive, Pseudomonas organisms are generally susceptible to a variety of antibiotics, including aminoglycosides and fluoroquinolones,” says Chistopher J. Rapuano, MD, director of cornea services at Wills Eye Hospital in Philadelphia. Early diagnosis and treatment with intensive topical antibiotics early in its course—when it just involves the cornea—often provides rather good results, according to Dr. Rapuano. However, “when the infection reaches the sclera, the clinical results are typically much worse,” Dr. Rapuano says, echoing Dr. Donnenfeld’s conclusion. “Topical antibiotic therapy just isn’t as effective in eyes with infectious scleritis.”
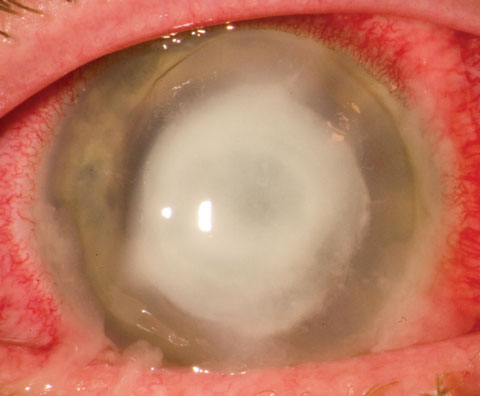 |
| Keeping Pseudomonas ulcers, such as this one, from extending into the sclera is paramount. Photo: Christopher Croasdale, MD |
The Ghosts of Treatment Past and Present
“Years ago,” notes Dr. Rapuano, “most eyes with Pseudomonas scleritis were lost.”
Over time, treatment moved from cryotherapy—an improvement on earlier treatments, but still largely ineffective—to systemic fluoroquinolones, which “penetrate the eye rather well,” says Dr. Rapuano. “Doctors began using these medications in eyes with Pseudomonas scleritis when they became available in the United States in the late 1980s. The success in treating Pseudomonas scleritis dramatically improved.”1,2
Now, “therapy for this type of case might involve the use of topical gram-negative medications such as fluoroquinolone or aminoglycoside every 30 minutes,” says Dr. Donnenfeld. “Oral or even IV medications are used, and some specialists will even lavage the subconjunctival space with antibiotics.” Both doctors generally agree that moxifloxacin 400mg per day is the most common oral antibiotic used to treat Pseudomonas scleritis. “Oral fluorquinolones,” says Dr. Donnenfeld, “achieve tissue levels as high as IV medications, which makes them a good choice. However, IV delivery is required when an antibiotic such as the aminoglycoside tobramycin is preferred.” Additionally, “hyperbaric oxygen therapy has been attempted in some research facilities, and riboflavin UV crosslinking can be a very effective adjunctive therapy.”3 Crosslinking, Dr. Donnenfeld adds, “is generally reserved for resistant organisms such as fungi or resistant bacteria.”
With all this in their wheelhouse, eye care providers still lack a panacea and, “while it is certainly not successful in all cases, the current use of systemic fluoroquinolones has significantly improved our treatment of Pseudomonas scleritis,” says Dr. Rapuano. Today, eye care providers have a much more effective set of tools at their fingertips, and prevention and early diagnosis are ideal. “The best treatment of a limbal Pseudomonas ulceration,” posits Dr. Donnenfeld, “is to prevent it from spreading into the sclera.”
|
1. Eiferman RA. Cryotherapy of Pseudomonas keratitis and scleritis. Arch Ophthalmol. 1979;97(9):1637-9. 2. Cunningham MA, Alexander JK, Matoba AY, et al. Management and outcome of microbial anterior scleritis Cornea. 2011;30(9):1020-3. 3. Price MO, Tenkman LR, Schrier A, et al. Photoactivated riboflavin treatment of infectious keratitis using collagen cross-linking technology. J Refract Surg. 2012;(10):706-13. |
