 |
In our last column ("Concussion and Chronic Traumatic Encephalopathy"), we described chronic traumatic encephalopathy (CTE) as a progressive neurodegenerative disease that occurs in association with repetitive mild traumatic brain injury (mTBI).1 Concussion, while likely related to mTBI, is a separate and distinct condition characterized by trauma-induced alterations in a patient’s mental status.2,3
Although the majority of CTE patients report a history of concussions, it’s not a prerequisite for diagnosis, suggesting that even sub-concussive hits are sufficient to lead to CTE. The chronic and repetitive nature of the head trauma sustained, often in certain sports and military activities, is the most important driver of CTE.3,4 Research suggests tau protein pathology occurs uniquely in those regions of the brain that are most susceptible to stress during trauma.1,2,5,6
Research has also found CTE-associated pathology in the retina, primarily in the ganglion cell layer.7 Patients who have suffered an acute concussion commonly report symptoms of visual blur, field loss, diplopia and photosensitivity. Ophthalmic sequelae associated with concussion, TBI and CTE can be visually debilitating and may be sight threatening.
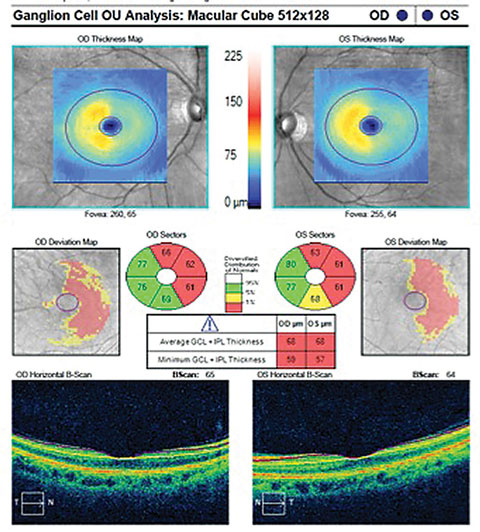 |
| OCT Macular cube with ganglion cell analysis in a post-TBI patient shows a distinct pattern of thinning in each eye. Image: Brad Sutton, OD. |
On-site Care
Concussion requires prompt clinical attention. After sustaining a possible concussion, athletes should immediately be removed from play (Table 1). Once an mTBI has occurred, the brain is in an extremely vulnerable state and is highly susceptible to additional injury. If a second concussion is experienced before the initial one has resolved, this could result in a potentially fatal brain swelling called second impact syndrome. This is why it is extremely important for athletes still experiencing signs and symptoms of a concussion to avoid risky physical activity. Of all patients who suffer one or more concussions, 10% to 15% have symptoms that continue for three months or longer. These patients are classified as having post-concussion syndrome.2,3,4
Table 1. Diagnosing Concussion3,4A suspected diagnosis of concussion may include features of the following clinical domains: Symptoms may be somatic (e.g., headache), cognitive (e.g., feeling as if in a fog) or emotional (e.g., mood changes). Physical signs (e.g., loss of consciousness, amnesia). Behavioral changes (e.g., irritability). Cognitive impairment (e.g., slowed reaction times). Sleep disturbance (e.g., drowsiness). If any one (or more) of these components is present, clinicians should suspect a concussion and institute the appropriate management strategy. |
Concussion is not a structural change, but rather a metabolic abnormality and therefore not detectable with radiologic studies. Although the detailed neuro-anatomy of concussion is beyond the scope of this column, it is essential clinicians recognize that it involves the cerebral cortex, brainstem and cerebellum. Many pathways are vulnerable, especially those that involve the coordination of movements, and it is logical to assess concussion by evaluating eye movements.
The King-Devick Test (KDT), often used to assess concussion, evaluates saccadic eye movement, which may alert the clinician to a cerebellar disturbance. The test yields an evidence-based, objective, physical measure for determining remove-from-play, thus preventing the cycle of brain re-injury and facilitating prompt entrance into the health care system.8,9 The procedure is fast, reliable and reproducible, all ideal attributes for sideline screening. According to one study involving boxers and mixed martial arts fighters, the KDT is an accurate and reliable method for identifying athletes with head trauma and concussion.8
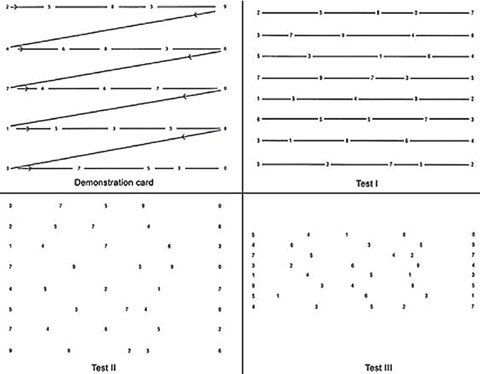 |
| The King-Devick test evaluates saccadic eye movements and may be used on-site when concussion is suspected. |
Cornerstones of Concussion Management
The mainstay of concussion management is physical and cognitive rest until symptoms resolve. This is followed by a graded program of exertion prior to medical clearance and return to playing (Table 2). The majority of symptoms related to the head injury will recover spontaneously over several days. During this period of recovery (while symptomatic), it is important to emphasize to the athlete the necessity of both physical and cognitive rest. Activities that require concentration and attention (e.g., scholastic work, video games, text messaging) may exacerbate symptoms and possibly delay recovery.
One study recently described the beneficial effects of post-concussion optometric care. In addition to traumatic structural damage to ocular tissues, patients may present with vergence disorders such as convergence insufficiency, accommodative deficits, fusional instability, oculomotor dysfunction and photosensitivity. Treatment methods may include tinted spectacle correction for full-time wear and conventional oculomotor-based vision therapy. Clinicians should consider a comprehensive optometric approach, as research suggests the injured, young-adult brain has considerable residual visual system plasticity.10
Table 2. Graduated Return To Play Protocol4Stage 1: No activity—complete physical and cognitive rest. Stage 2: Light aerobic exercise such as walking, swimming or stationary cycling. Stage 3: Sport-specific exercise such as skating and running drills. Stage 4: Non-contact drills such as passing or receiving in football. Stage 5: Full contact practice following medical clearance. Stage 6: Return to play—normal game activities. |
Concussion, mTBI and CTE are complex neurological conditions that share the common feature of traumatic injury. As the research continues to evolve, optometrists have the opportunity to “get in the game” and help people who are living with these challenges.
Dr. Wolter is in private practice in the Northeast region of Pennsylvania.
|
1. Stern RA, Daneshvar DH, Baugh CM, et al. Clinical presentation of chronic traumatic encephalopathy. Neurology. 2013;81(13):1122-9. 2. Stein TD, Alvarez VE, McKee AC. Concussion in chronic traumatic encephalopathy. Current Pain and Headache Reports. 2015;19(10):47. 3. Quality Standards Subcommittee. Practice parameter: the management of concussion in sports. Neurology. 1997;48:581-5. 4. McCrory P, Meeuwisse W, Johnston K, et al. Consensus statement on concussion in sport: The 3rd International Conference on Concussion in Sport Held in Zurich, November 2008. Journal of Athletic Training. 2009;44(4):434-48. 5. Verweiji BH, Muizelaar JP, Vinas FC, et al. Mitochondrial dysfunction after experimental and human brain injury and its possible reversal with a selective N-type calcium channel antagonist (SNX-111). Neurol Res. 1997;19:334-9. 6. Lei P, Ayton S, Finkelstein DI, et al. Tau protein: relevance to Parkinson’s disease. Int J Biochem Cell Biol. 2010;42(11):1775-8. 7. Slick N. The ocular manifestations of chronic traumatic encephalopathy. ProQuest Dissertations & Theses Global. 2014. Available at http://search.proquest.com/docview/1560235964. Accessed February 2, 2017. 8. 8. Galetta KM, Barrett J, Allen M, et al. The King-Devick test as a determinant of head trauma and concussion in boxers and MMA fighters. Neurology. 2011;76(17):1456-62. 9. Dhawan P, Starling A, Tapsell1 L, et al. King-Devick Test identifies symptomatic concussion in real-time and asymptomatic concussion over time. Neurology. 2014;82:10. 10. Tannen NM, Tannen B, Ciuffreda KJ. Optometric management of a post-concussion patient: a case report. Vision Dev & Rehab. 2016;2(4):237-42. |
