 |
|
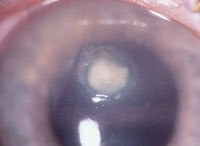
A suspicious white lesion was visible on this contact lens wearer’s cornea.
How should you manage this patient? |
 |
|
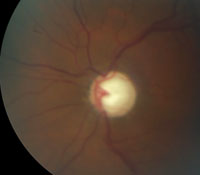
This 42-year-old patient exhibited advanced cupping in both eyes.
|
|
|
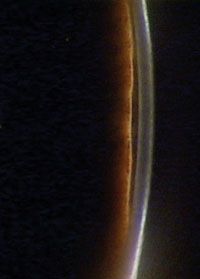
Gonioscopic view of the patient’s angle. What’s causing this patient’s glaucoma?
|
 |
|
This patient had sudden floaters and decreased vision. Fundus exam showed blood in the vitreous. What could have caused it? And what do you do about it?
|
It’s time to refer the patient.
Not that long ago, such a referral meant you’d never see the patient again. The corneal specialist would take charge—and take the patient. But, if you send the patient to an optometric referral center, that’s no longer the case. The patient will return to you for follow-up comanagement, explains Christopher Quinn, OD, president of one such referral center, Omni Eye Services of New Jersey, in Iselin, NJ.
To be an active partner in a comanagement arrangement—and indeed to lead the effort—you’ll need to be able to size up all the patient care options, including those you may have to coordinate with another doctor.
Four leaders in optometric comanagement offer their views of how they’d manage several tough cases that have presented a conundrum to either an optometric referral center or to practitioners who refer patients in to the comanagement center. Learning the ins and outs of complex cases that involve more than one eye care professional will better prepare you to direct the course of patient care in comanagement situations, so that the patient remains a part of your practice.
Call in the Calvary for Corneal Ulcer?
• Diagnostic data. A 26-year-old white female presented to her optometrist with a complaint of significant pain in the right eye that had lasted for a day. She reported that her pain had worsened after she took out her soft contact lenses that morning. Best-corrected acuity in that eye was 20/40. A suspicious white lesion was visible on her cornea. How should you treat this young patient?
• Discussion. It’s not strange that the patient reported feeling worse after removing the contacts. “It’s like a bandage essentially, and that’s where it just keeps getting worse,” says Brian Den Beste, OD, founder of Lasik Pro Eye Consultants in Orlando, Fla. To avoid further problems, reiterate that she needs to discontinue wearing her lenses.
Next, culture the eye to figure out whether the lesion is an infectious ulcer or sterile inflammatory infiltrate. If you’re not equipped to perform the culture and suspect it could be more than a simple infiltrate, refer the patient to someone who can.
But, don’t wait for the culture results before starting the patient on antibiotics. “This is an infection until proven otherwise,” says Daryl Mann, OD, chief manager of SouthEast Eye Specialists in Tennessee. “If you look at the anterior chamber and you see too many cells to count, it points to an infectious etiology, along with the pain and appearance.”
Dr. Mann says it’s never a mistake to put the patient on a broad-spectrum antibiotic in the first 24 hours. You’ll likely have the lab results within a day or two, and then you can tailor therapy depending whether it’s gram-positive or gram-negative.
While all of the doctors agree that antibiotic treatment is the way to go, each has a different preference. Dr. Mann opts for fortified antibiotics from his compounding pharmacist—using 25mg/ml vancomycin and 14mg/ml tobramycin. He prescribes one on the hour and one on the half hour for the first 24 hours, with immediate follow-up the next day.
Dr. Den Beste, on the other hand, would prescribe a fluoroquinolone to be instilled every five minutes for the first 35 minutes or hour, and then every half an hour for the first 24 hours. “This class of drugs has changed the game since the 1990s,” he says. For instance, a recent 20-year review of multiple, head-to-head studies on fortified antibiotics vs. fluoroquinolones found no substantial difference in outcomes.1 These results, plus easy accessibility and affordability for patients, are the factors that make a fluoroquinolone Dr. Den Beste’s first choice.
Robert Vandervort, OD, director of Heartland Eye Consultants, in Omaha, Neb., would consider using Polytrim (polymyxin B/
trimethoprim, Allergan) or another adjunctive medication in addition to the fluoroquinolone. “When I culture these, I’m always surprised at how many times the cultures do come back that they show sensitivity to trimethoprim and polymyxin B,” he says.
Although the doctors vary in their approaches, they almost unanimously agree on one treatment you should avoid. “Probably the biggest mistake clinicians make is to put steroids on an unidentified ulcer,” Dr. Den Beste says. “You’ll make the patient feel better, but you’re really helping the bug, particularly in fungal cases.”
There’s always been some controversy about using steroids when managing infectious keratitis, presumably to prevent scarring and vision loss. However, the Steroids for Corneal Ulcers Trial (SCUT) found that adjunctive topical corticosteroid use did not improve three-month vision in patients with bacterial corneal ulcers.2 “We’re not too worried about lessening that scarification, at least in my mind. It’s more about saving an eye,” Dr. Den Beste says. “We’re trying to put out the fire; we’re trying to keep the cornea from perforating.”
To do that, you’ll want to watch this patient like a hawk—see her back within a day and follow up often. And if in doubt, refer it out. But send to a corneal specialist if available, so that targeted care can be provided, knowing that long-term management will revert back to your practice.
Two Bottles Too Many
• Diagnostic data. A 42-year-old black male treated by his optometrist for primary open-angle glaucoma (POAG) for the past four years presented without complaints. His current medications included Lumigan (bimatoprost, Allergan) QD OU, Cosopt (dorzolamide/timolol, Merck) BID OU, and Alphagan P (brimonidine, Allergan) BID OU. His family history was significant; his grandmother was treated for glaucoma prior to her death.
The patient’s best-corrected visual acuity was 20/20 OU. He had a slightly thin cornea, with pachymetry readings of 539µm OD and 529µm OS. His intraocular pressure measured 14mm Hg OD and 16mm Hg OS. His slit-lamp exam was unremarkable.
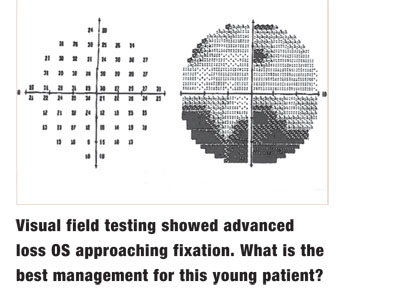
Imaging showed advanced cupping in both eyes. Visual field testing showed advanced loss OS approaching fixation.
What is the most appropriate management for this young glaucoma patient?
• Discussion. When three bottles are needed to control IOP, the question becomes: Is the patient on too many medications? As the number of medications increases, studies have shown non-compliance becomes a big concern.3-5
 Maximum medical therapy in patients with POAG generally means a prostaglandin and a combination drug such as Cosopt or Combigan (brimonidine/timolol, Allergan), says Dr. Vandervort. “Once you start getting to a third medication, your back is against the wall,” he says. “You can have a patient on three different medications but compliance goes way down. If I have someone on a prostaglandin of some kind and then add Cosopt or Combigan, we’re getting close to the end of medical therapy.”
Maximum medical therapy in patients with POAG generally means a prostaglandin and a combination drug such as Cosopt or Combigan (brimonidine/timolol, Allergan), says Dr. Vandervort. “Once you start getting to a third medication, your back is against the wall,” he says. “You can have a patient on three different medications but compliance goes way down. If I have someone on a prostaglandin of some kind and then add Cosopt or Combigan, we’re getting close to the end of medical therapy.”
Considering the patient’s relatively young age, family history and multiple medications, continuing this course of medical polytherapy is not a long-term solution and surgical intervention should be pursued—especially if there is any hint of progression, says Dr. Mann.
Once you make the decision, your comanagement role should include recommending that the patient undergo surgical intervention as soon as possible, the doctors suggest.
But the surgical options vary. Selective laser trabeculoplasty (SLT) is often the first surgical choice for most glaucoma patients. However, SLT may not be the best course of action in this case, Dr. Quinn says. “We don’t have a lot of time for this patient,” he says, noting that while the risks associated with SLT may be quite low, “there is also a risk we could further delay a more appropriate intervention for this patient that would really get his pressure where we need it.”
Other surgical options for this patient include trabeculectomy with mitomycin (MMC) or a tube shunt procedure, Dr. Quinn adds.
The Tube Versus Trabeculectomy (TVT) study found the two procedures are almost equivalent in terms of IOP lowering.6 “So, in my mind, a tube is probably a better option for this patient, since there is a lower risk of failure,” Dr. Quinn says.

If a patient must wait for surgical intervention at a busy clinic, consider prescribing an oral carbonic anhydrase inhibitor in the interim, such as a half-tablet of Diamox (acetazolamide, Duramed) TID, says Dr. Den Beste. “It’s a great drug to get the IOP down short-term,” he says.
Look at Glaucoma from Every Angle
• Diagnostic data. A 66-year-old white female was referred for an evaluation of her glaucoma status. Upon examination, her best-corrected visual acuity was 20/25 OU, and she had a mild cataract. She had no afferent pupillary defect in either eye. Pachymetry readings showed normal corneal thickness. Medications included a prostaglandin analog, yet her IOP measured 29mm Hg OD and 28mm Hg OS. Her visual fields were full.
What’s causing this patient’s glaucoma?
• Discussion. If you think this patient has undergone all the necessary tests, think again. In this patient’s case, further examination with gonioscopy revealed she had angle-closure glaucoma.
Gonioscopy is an art many optometrists and ophthalmologists don’t employ, but it’s a critical tool in the initial evaluation of a glaucoma patient, particularly the primary open-angle glaucoma patient, Dr. Mann says. However, fewer than half of clinicians perform gonioscopy during the initial evaluation of primary open-angle glaucoma.7 Gonioscopy can also assist in the diagnosis of pseudoexfoliation, pigmentary glaucoma and comparing a healthy angle vs. a diseased angle.
“Patients come in and primary care optometrists can’t consistently get them to respond to medication. And lo and behold, you look with a gonioscopy lens, and you don’t see any angle structures,” Dr. Mann says.
As a long-term glaucoma patient develops cataracts, an open but narrow angle can actually convert over to a chronic angle-closure state during a period of 10 to 20 years, says Dr. Quinn.
“It’s amazing how long an angle can survive before it gives up the ghost and causes pupillary block,” says Dr. Den Beste. As such, preventative care is essential. “I had a patient with cataracts. She was wearing a +8.00D sphere and had gone her whole life without angle closure. She had cataract surgery and was so happy. But a few years go by and she comes back with a steamy cornea and a pressure of 50mm Hg—she had angle closure. So, just because the patient is pseudophakic doesn’t mean that peripheral anterior synechiae can’t occur. That’s a rare case, but clearly we need to put that gonio prism on these patients more often.”
Just how often should gonioscopy be repeated? For patients with a grade 3 or 4 angle to start, Dr. Vandervort will repeat gonioscopy every few years.
However, for patients with recurrent uveitis, he performs gonioscopy once or twice a year. “Those angles can trick you. It happened to me one time,” he says. “I wasn’t paying attention to doing repetitive gonioscopy on a chronic uveitis patient and her angles zippered shut. And uveitic glaucoma due to angle closure is a mess to take care of.”
Anterior segment OCT is an additional test that can help a clinician examine angle configurations and document whether an angle is at risk for occlusion, Dr. Mann says. “Explaining a prophylactic iridotomy for a narrow angle is one of the most difficult discussions to have with a patient (for them) to understand why we are doing surgery when there’s not really a problem now, but they may have a problem in the future. Having that OCT to show them helps.”
Even so, OCT should not replace gonioscopy, he adds. If this skill is not in your wheelhouse, start practicing on staff members and patients, and get comfortable with a test that is a basic part of the optometric exam.
Don’t Let Sudden Floaters Slide
• Diagnostic data. A 56-year-old white male reported to his optometrist that he had been experiencing sudden floaters and decreased vision OS for the past day. He denied having any photopsia, or any previous trauma or comparable episodes.
Best-corrected visual acuity was 20/20 OD and 20/40 OS, with no afferent pupillary defect. Visual confrontation fields were full, and the slit-lamp examination was normal. A fundus exam of the left eye showed blood in the vitreous.
What could be causing this vitreous hemorrhage?
• Discussion. “Always use caution in making a presumption that this is related to a vitreous detachment,” Dr. Quinn says. If your patient has venous-occlusive disease, diabetic retinopathy, sarcoid, retinopathy of prematurity or sickle-cell disease, you could be looking at bleeding caused by retinal neovascularization. It could also be blood from an adjacent source, such as macroaneurysms, tumors or choroidal neovascularization.
But, you’re most likely dealing with a posterior vitreous detachment (PVD) with a small surface vessel that broke.
Regardless, all four doctors agree you need to see the patient immediately to make sure. If your patient does have a PVD, your next concern is to look for a retinal tear. “Most of the time, when you have blood in the eye, your expectations of tears go way up,” Dr. Den Beste says. “And you don’t want to miss a tear because it can lead to a retinal detachment, which of course is a much more serious condition.”
Concern is warranted. About 15% of patients who present with acute, symptomatic PVD have a retinal tear—and as many as half have more than one.8 When vitreous bleeding is present with acute PVD, the incidence of retinal tears jumps to 70%.8
Carefully examine the vitreous for pigment: Shafer’s sign is an indicator of a retinal tear. You’ll also need to take a close look at the peripheral retina. The doctors recommend a 360° exam with binocular indirect ophthalmoscopy (BIO) and scleral depression. For the best view, have the patient recline or lie down in the exam chair, Dr. Mann says.
If the patient has a small pupil, a 30D lens may be helpful for better visualization. Dr. Vandervort also suggests using a three-mirror fundus lens for a more detailed view. “I am amazed at how many times I will find a small tear with a three-mirror lens that I missed on BIO,” he says. This may take a little extra time, but it’s worth the effort.
Also, look in the other eye. “You might get a better view without the vitreous hemorrhage to see if this patient has risk factors,” Dr. Den Beste says. But if you’re not able to get a good look, he stresses that you shouldn’t hesitate to refer the patient to a retinal specialist for further evaluation.
Even if you don’t detect any tears in a patient with acute PVD initially, don’t rule out the possibility of a late retinal tear. Diligent follow-up is just as crucial as careful diagnostic evaluation with vitreous hemorrhage.
Schedule follow-up within seven to 10 days, but emphasize that patients need to see you immediately if symptoms worsen or they experience any changes, i.e., more floaters or obscuration of vision.
“If you get new people on staff, make sure they understand the protocol for symptoms and the protocol for follow-up,” Dr. Den Beste says. “A leading cause of malpractice in eye care is inappropriate scheduling of the patient.”
A little tear is an easy fix compared to a vitrectomy or retinal detachment repair, he says. Early identification and active oversight at your clinic could limit the need for a retina specialist to perform more risky, interventional procedures later. n
This article was adapted from the Special Session, “Comanagement Conundrums,” at SECO 2014, which was sponsored by VSP. However, this article has no commercial sponsorship.
1. Hanet M, Jamart J, Chaves AP. Fluoroquinolones or fortified antibiotics for treating bacterial keratitis: systematic review and meta-analysis of comparative studies. Canad J Ophthalmol. 2012 Dec;47(6):493-9.
2. Srinivasan M1, Mascarenhas J, Rajaraman R, et al. Corticosteroids for bacterial keratitis: the Steroids for Corneal Ulcers Trial (SCUT). Arch Ophthalmol. 2012 Feb;130(2):143-50.
3. Robin AL, Covert D. Does adjunctive glaucoma therapy affect adherence to the initial primary therapy? Ophthalmology. 2005 May;112(5):863-8.
4. Dasgupta S, Oates V, Bookhart BK, et al. Population-based persistency rates for topical glaucoma medications measured with pharmacy claims data. Am J Manag Care. 2002 Aug;8(10 Suppl):S255-61.
5. Spooner JJ, Bullano MF, Ikeda LI, et al. Rates of discontinuation and change of glaucoma therapy in a managed care setting. Am J Manag Care. 2002;8:S262-0.
6. Gedde SJ, Schiffman JC, Feuer WJ, et al; Tube versus Trabeculectomy Study Group. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012 May;153(5):789-803.
7. Fremont AM, Lee PP, Mangione CM, et al. Patterns of care for open-angle glaucoma in managed care. Arch Ophthalmol. 2003 Jun;121(6):777-83.
8. Sharma MC, Regillo CD, Shuler MF, et al. Determination of the incidence and clinical characteristics of subsequent retinal tears following treatment of the acute posterior vitreous detachment-related initial retinal tears. Am J Ophthalmol. 2004 Aug;138(2):280-4.
