
From the Desk of The President
 I am excited to present our first OCCRS quarterly newsletter. Organized in 2002 and chartered in 2004, the Optometric Corneal, Cataract and Refractive Society is optometry’s voice in the field of refractive surgery, comanagement and other technologies designed to alter the refractive status of the human eye. Our mission is to bring together optometrists and researchers with an interest in refractive technologies, and provide a forum for education and interaction. We host an annual symposium to share our expertise and enthusiasm for all things refractive.
I am excited to present our first OCCRS quarterly newsletter. Organized in 2002 and chartered in 2004, the Optometric Corneal, Cataract and Refractive Society is optometry’s voice in the field of refractive surgery, comanagement and other technologies designed to alter the refractive status of the human eye. Our mission is to bring together optometrists and researchers with an interest in refractive technologies, and provide a forum for education and interaction. We host an annual symposium to share our expertise and enthusiasm for all things refractive.
OCCRS gives us a forum for discussion and allows us to present ourselves as the key players in supporting patients interested in altering their refractive status. Our members can then act as a resource for our colleagues who are not directly involved in refractive surgical care, but whose patients seek such care. We support collaborative care with surgeons for the benefit of our patients.
Our goals include:
- Establish a home for optometric clinicians, researchers and business owners in the field of refractive technologies
- Develop and deliver scientifically-based educational programs on refractive technology for optometrists
- Act as a resource to optometric organizations, schools and colleges of optometry, and educational meetings for matters and information regarding refractive technologies
- Encourage research in the field of refractive technology, and create a forum to present that research through lectures, papers and poster presentations
Our mission statement: To advance the art and science of refractive technology and the knowledge and skills of optometrists participating in refractive technology as well as provide clinical and practice management education to optometrists through various forms of communication and forums.
We look forward to working with our colleagues to advance comanagement of corneal and cataract procedures, and promoting new technologies to benefit our patients.
Tracy Schroeder Swartz, OD, MS, FAAO, Dipl ABO,
President, OCCRS
Annual Meeting

The 16th annual OCCRS symposium took place from April 13 to 14 in San Diego, California.
The Optometric Cornea, Cataract and Refractive Society’s annual symposium took place in San Diego, Calif., April 13 to 14. This was our 16th meeting, and we continued to combine lectures with panelists and workshops showcasing new technologies. Topics included candidacy for a full spectrum of vision correction procedures, postoperative protocols, endothelial surgery updates, perioperative ocular surface disease, management of irregular astigmatism and an update on MIGS procedures.
![]()
Cornea, Cataract and Refractive Surgery Management

Make sure to educate patients needing toric lenses early to make the discussion prior to referral easier.
Thinking Refractively
The Optometric Cornea, Cataract and Refractive Society is a refractive-based group, but we are not focused solely on LASIK. While optometrists often think about refractive endpoints for glasses and contacts, they are less familiar with maximizing visual aspects of ocular surgery. However, they will find that examining and commenting on the state of the lens for patients 50 years and older will increase familiarity with cataract surgery for both themselves and the patient.
“A baby cataract” or a “toddler cataract” will later become “time for cataract surgery.” Starting the conversation early with patients means they will not be shellshocked to hear the term “cataract.” Make sure to educate patients needing toric lenses early to make the discussion prior to referral easier. Premium lenses are more attractive when the patient has years to consider their options and save the required funds.
An important aspect of comanagement is consideration of the refractive endpoint. Most surgeons default to distance correction, targeting plano. But myopes may prefer to remain nearsighted and wear correction for distance. We know our patients best and need to look out for their visual needs. Determine this important consideration prior to surgery to avoid extremely unhappy patient postoperatively. Discussing this option years before surgery allows patients to carefully consider their options and feel more reassured when the cataract requires extraction. In addition, fitting patients in multifocal contacts is an excellent method to demonstrate multifocal intraocular lens options. Demonstration of monovision or a multifocal correction should be initiated prior to referral to the MD. Read more.
![]()
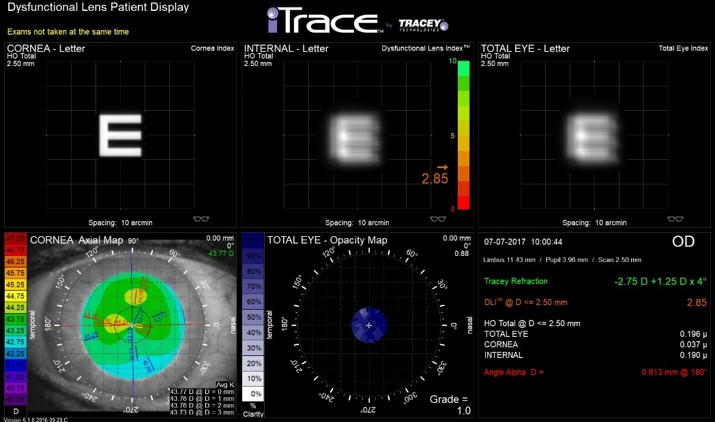
This iTrace display (Tracey Technologies, Houston, TX) demonstrates the effect of the healthy external cornea (clear, left “E”), cataractous lens (blurry, middle “E”) and overall vision (blurry right “E”). This patient’s blurry vision is due to the cataract, and this patient is read for surgery. (Courtesy of Tracy Schroeder Swartz, OD, MS, FAAO, Dipl ABO)
Is the Eye Ready for Surgery?
Patients’ options for vision correction have advanced considerably. Not only do we have wavefront-guided and wavefront-optimized LASIK, we now have topography-integrated as well as topography-guided applications. These require higher order aberrations and topography information to be acquired for surgical planning. Ocular surface disease can affect these measurements and, subsequently, the outcomes.
Cataract surgery also requires corneal measurements. Biometry, or axial length measurement, is now performed optically rather than with ultrasound. Autokeratometry or topography used in intraocular lens (IOL) calculations is critical for strong outcomes and also may be influenced by ocular surface disease.
It is important to consider whether the patient you are referring for surgery is ready for these measurements. Treating ocular inflammation, lid disease including meibomian gland dysfunction and blepharitis, and corneal issues prior to referral ensures correct measurements and demonstrates clinical prowess to the surgeon. Consider addressing corneal issues such as EBMD, Salzmann’s degeneration or keratoconus prior to cataract surgery. This may be accomplished by referring to a corneal specialist for both corneal and cataract evaluation, or may require separate referrals. Read more.
![]()